Something I delayed from publishing from October 30th because I thought it’s not useful to anyone. However, in the light of recent talk of variants (B.1.1.529), I’m seeing the repeat of the same arguments which are flatly incorrectly from an empirical standpoint. Here’s another view I’m presenting where I’m trying to show that variants are neither benign nor are they a cause for discrimination against unvaccinated and most of all, they are certainly not a reason to “Boost”!.
Someone challenged the experts to explain and they folded. This is normal because they are uncomfortable with simple mathematics.
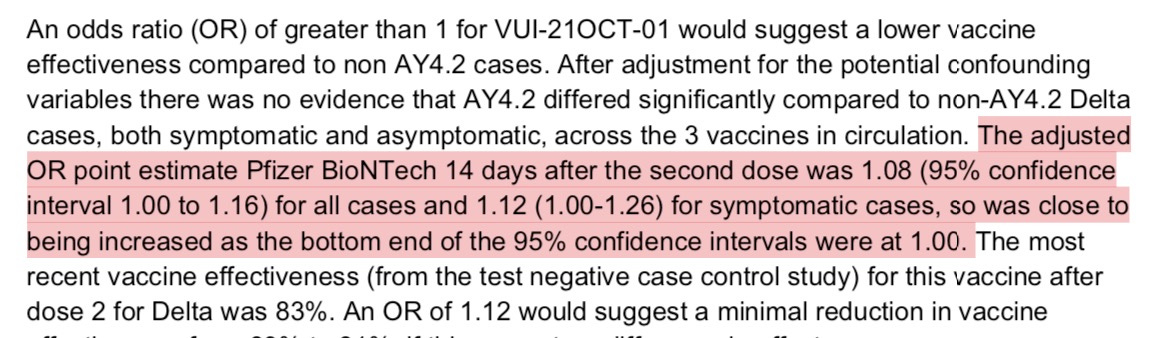
The uncomfortable truth, as hypothesized before: UK Report shows that Delta variant AY.4.2 is spreading even better in the vaccinated than unvaccinated.
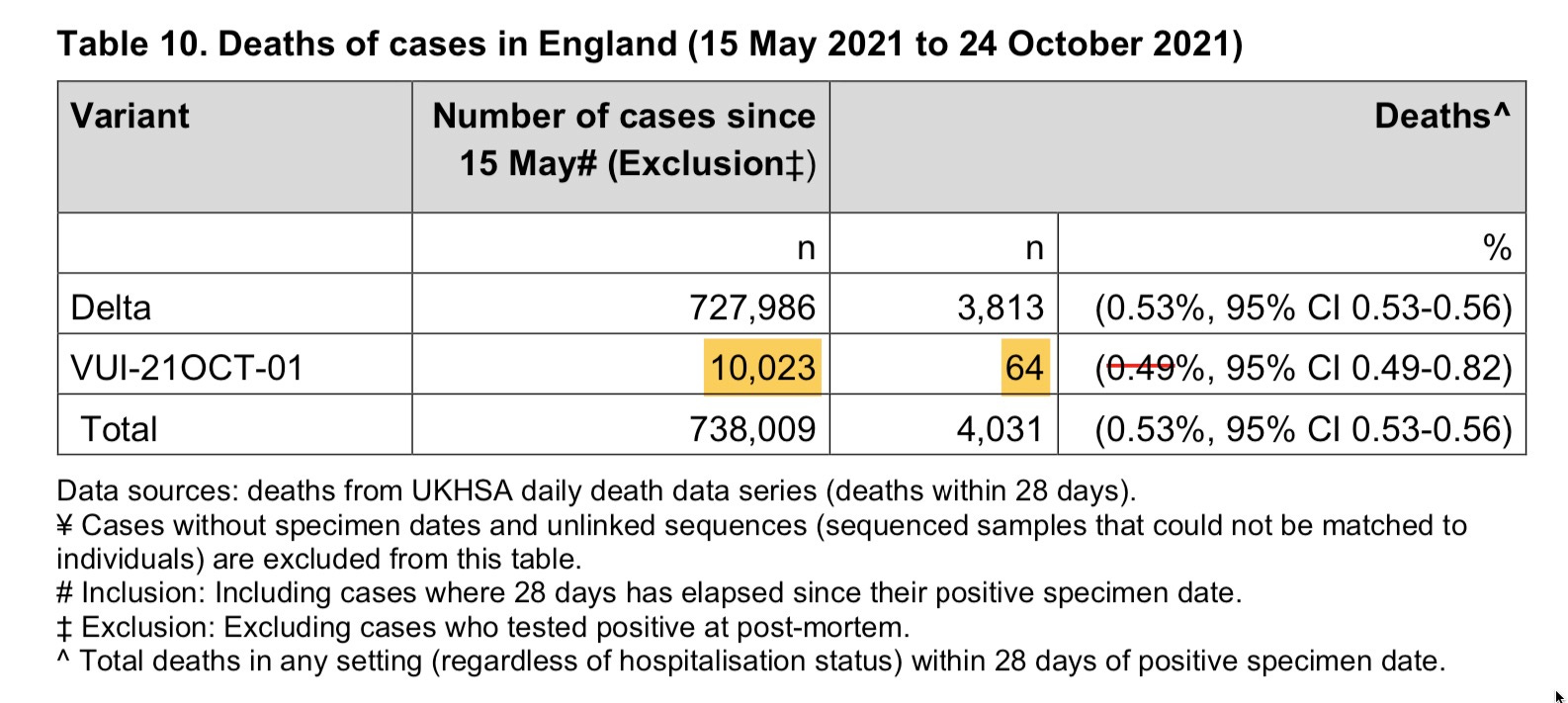
And it’s a higher death rate than what they’ve calculated of .49% which is the lower bound, upper being .82%
A conspicuous error which I will use to calculate the real death rate .64% in folks who got AY.4.2 since they refuse to release prior exposure stratified data.
It could be worse than that because we still don’t know
the years of life lost (YLL) for the dead subgroup.
Say we knew the YLL was higher for Delta-Plus, it would almost certainly mean it’s killing younger people and this could be a sign of higher lethality but being masked by crude death rates.
If the YLL is lower, it could mean it’s killing older people but at a faster rate, so it’s an example of a variant that’s found a niche and going for the lowest hanging fruit hard
If the YLL is the same then it’s a situation where a breakup of who died would unhide any clusters. For example, say the kids who were recently vaccinated passed it on to their parents in the UK. Both demographics are seeing explosive rise of cases in the vaccinated. Then we would expect some deaths in that age group, as well as elderly.
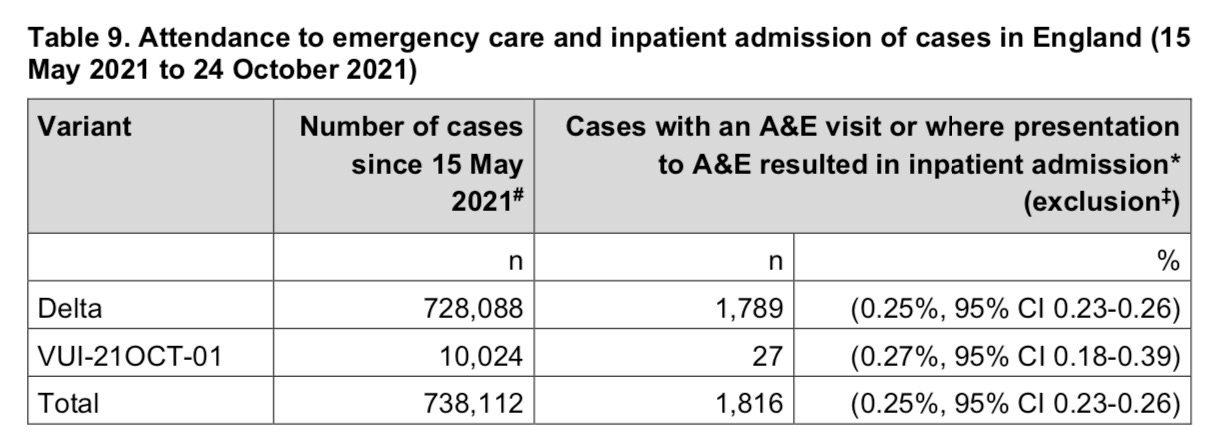
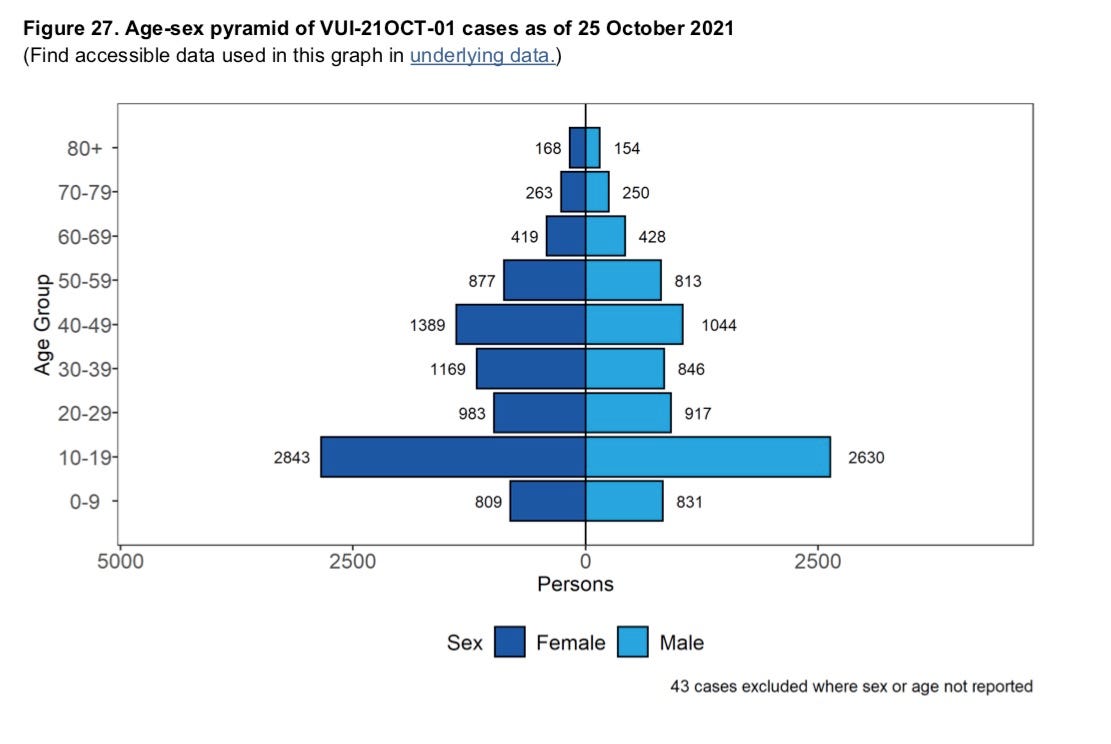
Notice The Following: Emergency Admissions Numbers same but higher deaths.
Exclusions include people who tested positive after they died which means they never even made it to the hospital.
This is not proof if variant becoming less virulent, it’s the opposite. And the only reason people are ignoring it because it disproportionately affects Vaccinated at the moment. Why is that so? Well. We’ll see soon enough.
“If our elderly die at home we will not tell you they died from a variant even if we swab and find out at post-mortem.”
We don’t ever stop the health authorities from lying to the public that the rise of variants within a sub-population is never the unvaccinated but the vaccinated! Here we see the attempt by UKHSA to pretend this is not a problem.
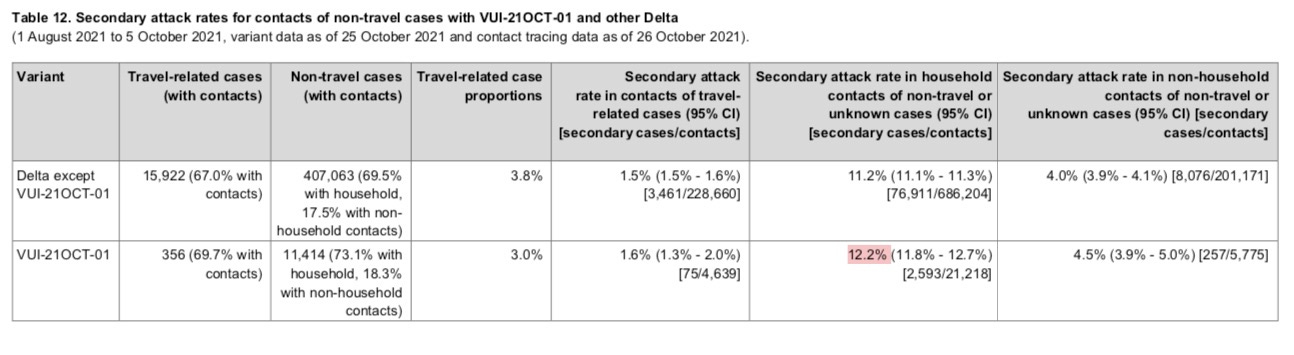
Secondary Attack Rates is higher for the variant. Why? Kids infecting moms not random travelers. This is due to homologous vaccine match (Pfizer). Not higher transmission but lower resistance to infection in vaccinated when challenged perpetually by viral shedding at high levels.
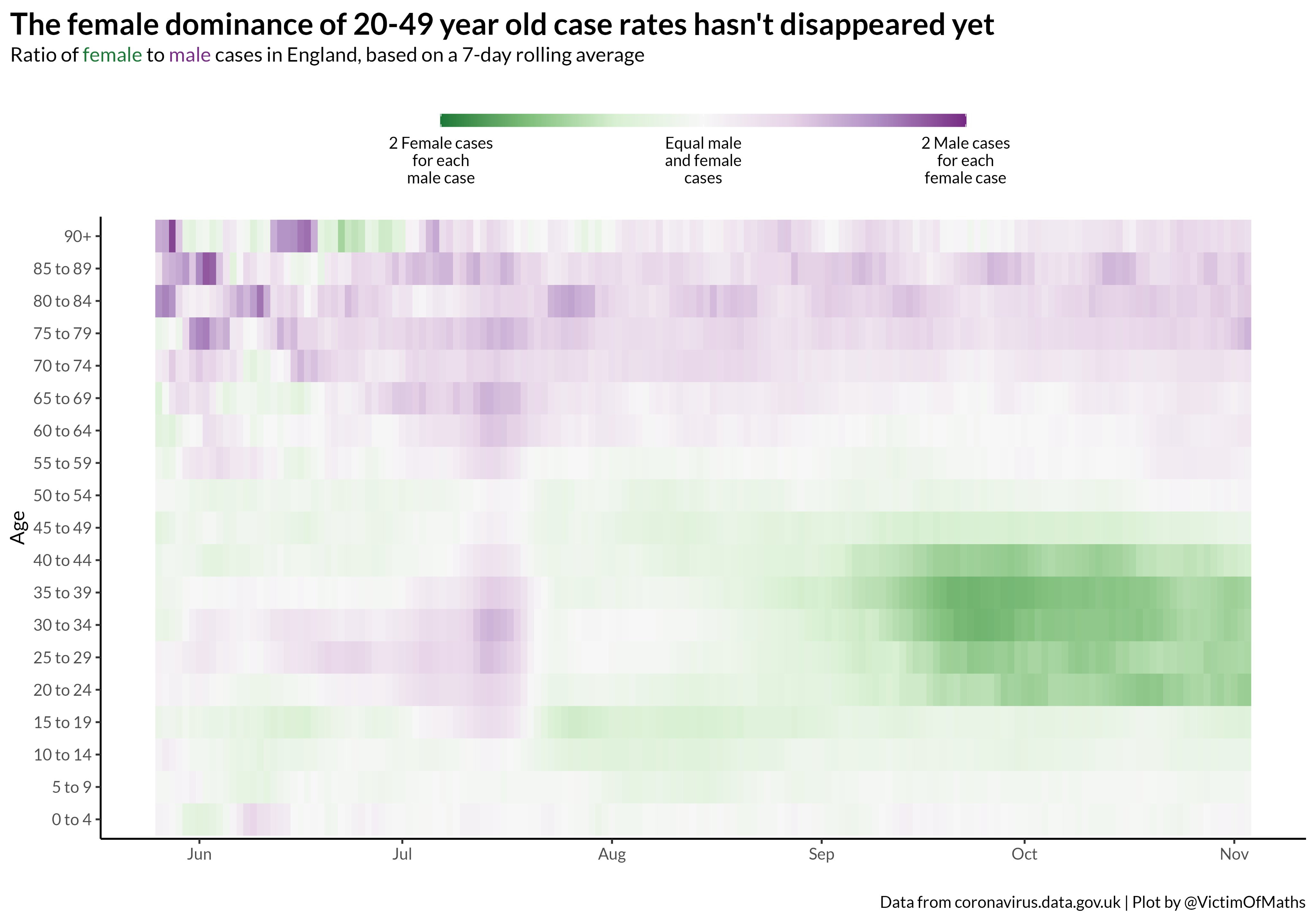
UK Infections by @VictimofMaths on twitter
We have to stop the fear mongers from misleading the public consistently. They will just use bad reasoning from the skeptical side as a straw man to further persecute and discriminate the people that never vaccinated and contributed to population level selection pressure.
Most importantly, we are pretending that the variants are not that bad when our own vaccinated family and friends are most likely to die from it and they will cover it up because they don’t want to tell people that transmission and selection happens in the vaccinated.
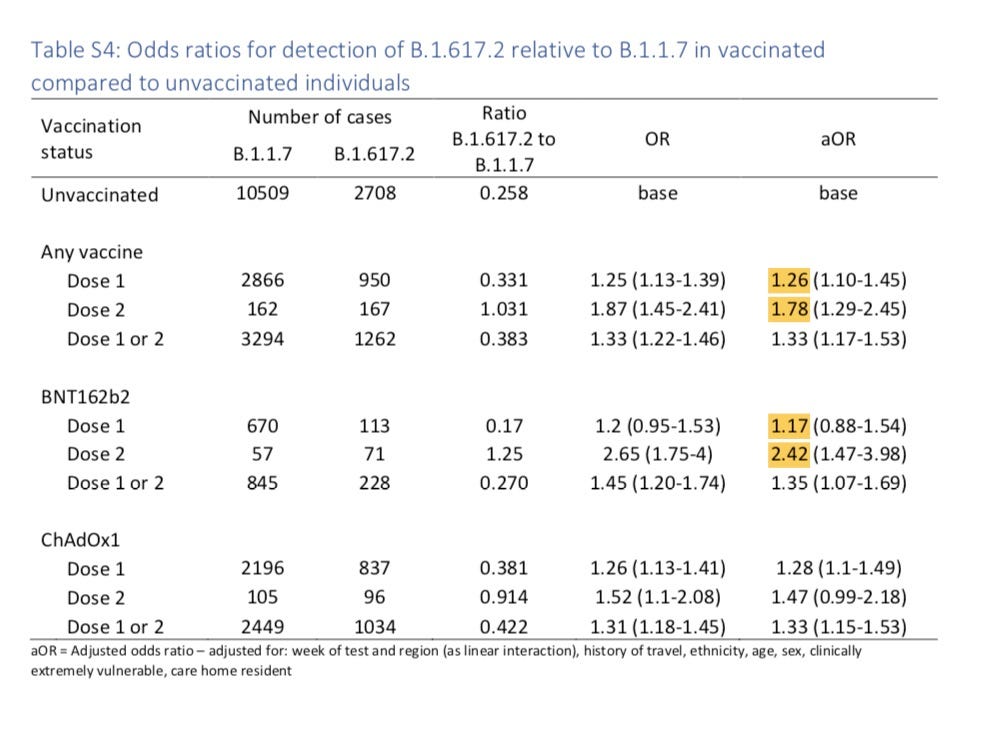
Here’s Delta odds ratio of infection from the Summer. Did you know that 2.42x higher chance of delta infection in Double vaccinated than unvaccinated? Why didn’t you know? Because we are being told that these variants are nothing for the vaccinated and only the unvaccinated spread them and the unvaccinated respond poorly by suggesting “it’s not that bad”.
Table from Supplement to: Lopez Bernal J, Andrews N, Gower C, et al. Effectiveness of Covid-19 vaccines against the B.1.617.2 (delta) variant. N Engl J Med 2021;385:585-94. DOI: 10.1056/NEJMoa2108891. https://www.nejm.org/doi/suppl/10.1056/NEJMoa2108891/suppl_file/nejmoa2108891_appendix.pdf
People who do not participate in coordinated mass application of drug pressure (people who haven’t been injected or infected) cannot conceivably play any role at all in the selection (cultivation, filtration) or the transmission (uninfected person cannot replicate or shed virus) of variants that achieve general fitness with respect to vaccinated population.
Resistance to a treatment can only be due to the people who participated in the mass exposure to the drug and the disease. This cannot be the case for the unvaccinated, it is by definition the Vaccinated and especially the FULLY vaccinated that contribute to this kind of evolution.
I welcome any feedback especially with respect to corrections and attribution.
Update!: I agree with this formulation by Dr. Malone.
This post is still under construction because I still have work left to do figuring out the role of incidence density change at the point of vaccination and seropositivity as an underlying risk, then onward transmission.
PS. Ethical Skeptic says this too on his Twitter re: Omicron. If mild..could be the end. Why do I have doubts? Hmmm. Will it crumble. Wouldn’t that be something
"In 2021, Berenson tweeted that COVID-19 vaccinations had led to 50 times more adverse effects than flu vaccine. PolitiFact rated the claim 'mostly false'.[6] The Atlantic called him 'The pandemic's wrongest man', owing to his false claims of the vaccine's ineffectiveness."
Thank you for sharing. Given I have no final formed “opinion” I tend to read many different ones..I already know the general narrative given by the government in coordination with various agencies and mainstream media. Since I cannot make snap judgments based on any opinion or theory—this crisis has been difficult to decipher because it is not binary having been caused by typical oversimplification of a subject. Even though it is happening.
So there seems to be an area of blending between the virtual world and the natural world. Like a hurricane that hit one area became every area even though the sky was sunny where you live. So the known became a belief that is ungrounded. Not empirical practically speaking. Data then if data is all we possess can be quantum and the quantifier’s view is not necessarily fact but becomes fact if believed. Yet the fact is not located in physicality because the presupposition that data is proof of fact is quantum-ly strange in a truly tantum scenario. Simply- location implies empirical fact giving data it’s useful purpose but not a universal one. In situations such as these..We must rely as humans on narrative—and our experience. But is that anecdote? Anecdote cannot necessarily be antidote because again what is the reality or philosophical governance believed by the “reporter”. I constantly recheck my own presuppositions especially as discrete facts alone become more and more nano. In our world the only Absolute is change whereas great faith is being required to accept the unseen. This causes a scientific religiosity in a community that once was driven more materialistically. Now it has become somewhat gnostic. Scientific Gnosticism. A separation between the body and the mind. The virus being an evil archon and the scientists some, the high priests of secret indecipherable knowledge.
There exists, a large reductionism to sift through for a simple person such as me. High complexity abiding only in data that is presupposed to be physical proof leaves an outcome that branches in multiple directions-and that is how the data “feels” both fractal and ouroborean if you could take a snapshot. And the template begins to look more and more like chaos which if consciously viewed as template looks like the collapse of everything. Such as when a pebble hits a windshield and gradually….well you know the rest. Misapplication of one size fits all..has resulted in chaos..
The hurricane is caused by data and undifferentiated emotion which tessellates seemingly infinitely in a bounded space.
Quite agree with your “this crisis has been difficult to decipher because ... typical oversimplification of a subject”. I came over here because of several comments by AlmostWrong on a Substack post by Alexandros Marinos on Scott Alexander’s “take-down” of the ivermectin studies posted by Ivmmeta:
AlmostWrong is certainly a prolific writer who imparts a lot of detailed statistics, most of which I really don’t follow. But I had to question his “Delta variant AY.4.2 is spreading even better in the vaccinated than unvaccinated.” Not sure what the source for that claim might be but offhand it seems that that might be due to the way the data is obtained. Maybe – I emphasize the term, maybe – there are more cases among the vaccinated than the unvaxxed simply because there are more of the former than the latter. Or maybe the vaxxed are more likely to get tested than the unvaxxed.
But regardless of how accurate that specific scenario may be, it seems that part of the problem is that the statistical data is probably subject to any number of confounding factors that are not at all easily quantified. And part of that problem may be that there’s no model of the mechanisms involved – something that Marinos touched on if rather briefly; that there’s no understanding of how ivermectin might contribute to the differences in the results over the more credible studies. Absent such models – apart from “worms!” – it seems rather difficult to determine if the statistical results make sense, are credible. As bad as doing phrenology without any model how different psychological traits might affect skull bumps and hollows.
Which is unfortunate as there is in fact some decent models available that may give an inkling of what’s “happening under the hood”. For instance, this NCBI article below shows that Ivermectin does, in fact, have some anti-viral effects. But those come from the fact that its target is "not a viral component, but a host protein important in intracellular transport". Entirely different chemistry from the Pfizer & Merck anti-virals under development.
But that kinda makes ivermectin somewhat toxic at the "half maximal inhibitory concentration" (IC50) level, and not particularly effective at the "highest regulatory approved dose of ivermectin" which is at least a thirtieth to a fiftieth less than that IC50:
However, as the article suggests, even at that much reduced level, it may be "key to enabling the body's immune system to begin to mount the full antiviral response before the infection takes control." And that benefit may well contribute to *some* of the differences in the Ivmmeta studies - even apart from the effects of possible worm infections.
But those benefits look to be marginal at best - entirely consistent with the concentration levels of recommended doses - and likely to manifest themselves to any great or noticeable degree only when the patient was more or less on death's doorstep. Which seems to describe many of the Ivmmeta tests in question.
Would be interesting to try creating a patient model that incorporates those effects to determine if they would be sufficient to explain many of the Ivmmeta test results.
"who imparts a lot of detailed statistics, most of which I really don’t follow."
I have to say I'm sorry I do a bad job of writing. If I am wrong, it makes my wrongness not spread far and wide due to poor presentation, which is a relief.
On the other hand, if I am right, I was hoping someone more intelligent, skilled or influential can piece things together and make it usable. Apparently that's not yet happened, and it could be because I'm not able to make my case and that my case is not right.
As for AY.4.2 spreading (like omicron or any variant), the odds of being infected with a variant of the dominant strain is higher for those who have had some prior exposure some version of the dominant strain. In the case of vaccination, there is acute exposure to the spike protein in most vaccines and whole virus in others. The reason why a variant spreads faster (shows increasing incidence) in vaccinated vs unvaccinated is because unvaccinated either have no exposure to the virus or have exposure to slightly different mutants of the virus. When a mutant want to spread, it has to make no adjustments when it faces successive hosts with a cloned vaccinated immune response [as it's been programmed to neutralize wuhan virus]. It cannot easily do this for unvaccinated because unvaccinated and uninfected have innate immune response that neutralize all variants except those which are more transmissible, and unvaccinated recovered all have seen some version of the prevailing mutants making them harder to re-infect. This leaves only the vaccinated vulnerable. What I tried to show is that the 12% advantage that AY.4.2 had in spreading in vaccinated was after adjusting for confounders and testing and that the real reason why it was spreading is because young children at schools who were exposed got vaccinated, caught the virus and then infected their parents while this didn't happen for unvaccinated because the viruses they got infected with were all slightly different from each other and hence added up to nothing in terms of dominance.
Dear AlmostWrong. I spent some time this pm reading your comments to others. It confirmed what I saw in you if seeing can be attributed to reading. While I work on a response to Steersman here is what I wrote:
Well, AlmostWrong impresses my simple mind because I though ignorant, discern in this work, that, AW does not presuppose, rather asks instead the questions which precede answers that require “asking before proceeding.” AW’s ego which is merely an adaptive acquired mechanism does not fully override his/her heart and natural will for health for others.
Dear Robin, I look forward to reading your replies and the resources you share. The will to learn and self-correct is strong because as your correctly sensed- I want nothing but better health for all without sacrificing anything in the process we collectively hold dear, rather strengthening and improving our reliance tools that will not sabotage our own abilities to make amends if this over and critically so if this is not over, and just the beginning.
“I have to say I'm sorry I do a bad job of writing.”
Doesn’t seem all that bad.🙂 Though I can sympathize – I’ve written and posted a number of articles thither and yon – Medium, The Post Millennial, various blogs, etc – and know how difficult it can be to put words to paper in a coherent and readable form. “Writing: Craft & Art” by Rivers gave me some pointers that you might look into, though there are many other such sources.
And a couple of times I’ve even contracted a professional editor for assistance, though that can get a bit expensive. In any case, the latest was for this essay on Wikipedia’s Lysenkoism that you might have some interest in:
Big fan of Wikipedia in general, but when it comes to sex and gender, their vaunted “neutral point of view” is in tatters.
“the odds of being infected with a variant of the dominant strain is higher for those who have had some prior exposure some version of the dominant strain”
That may well be the case, but I wonder if you have any sources from biological or medical sources that would justify that argument. Seems to me that if the statistical results are not consistent with the models of the underlying process then either the model is inaccurate and there are other processes and factors in play, or the statistical sampling and the inferences drawn from it are flawed.
Partly why I alluded to Marinos’ reference to mechanisms, the NCBI article on ivermectin blood concentration levels, and “worms”, all as relevant models that may have some bearing on the results of those Ivmmeta studies. Something that you with your “physics training” should appreciate. 🙂
Thank you for the tips. I will try my best to incorporate and look forward to reading your article. I'm poorly trained in Physics I must say, but I will promise you this, I will write a detailed article explaining everything but that I was hesitant because as I mention in other comments, it's not enough to have models and plausible mechanisms, what we need is raw data that satisfies equations not merely directionally (that is it's not important be to just right about whether the effect statistical or mechanistic exists in the direction specified) but also in calculable size. Put differently, it's not sufficient to show "worms" or "co-infections" prevalence and ivermectin use might free off resources to fight other infections, but to actually precisely define that if this were not the case then what we would see. In the case of ivermectin, if the utility is limited to indirect benefits of intestinal infections then we should be able to say with confidence that ivermectin will not be able to clear infections of other kinds. This allows us to produce counter-factual which can then be used to invalidate the exclusivity of mechanisms. For example: Here you can see ivermectin was used to cure a urinary tract infection in a chronically infected covid patient at day 56 of infection to day 60. The infection resolved but covid did not. https://www.nature.com/articles/s41467-021-26602-3/figures/1
In my case, before I make my case more clearly that will take much longer as I gather the empirical data to be 100% sure of what I am saying, I had to put out this information in a haphazard way so that I can clear up my conscience that I didn't wait too long and allowed perfect to be the enemy of good enough. Therefore, I've put out this information, I will explain it properly as I gather more data specifically reinfection by vaccination date and once I have that, I will be able to prove or disprove conclusively what I think is happening.
Out of desperation, I appealed to UKHSA to release this data here:
Next I will ask Danish Authorities in the next day or two after I have collected more data about reinfection prevalence.
Sorry for not being able to make my case, but if I am wrong, no problem. If I am right, I needed to get this information out as soon as I could so that other people who also understand what I am thinking can take action.
Thank you!~ It's very intriguing that China is by all appearances and actions, the last bastion still standing against Covid-19. Also intriguing that they were the first country where it broke out as well. Lot's of unexplained and undetermined observations. Will it crumble?
Will it crumble? China has the same big problems the rest of the world has….with a lot less water…but frankly? Dunno.
Anyway…
It’s a strong paper by Ethical Skeptic who I follow periodically. IMHO I think he proves his point(s) but it requires on my part a complete recalibration of the whole narrative or at least large portions of it. So the rest of the world followed China’s example using authoritarian measures based on error filled presuppositions. The timeline and transmission matter. I get that.
I notice however that Ethical Skeptic completely left out the MIC involvement with China in the “shared” research as noted in Ralph Baric’s correspondence records. Given ES was in Naval Intelligence I always look for omissions like that too.
























PS. Ethical Skeptic says this too on his Twitter re: Omicron. If mild..could be the end. Why do I have doubts? Hmmm. Will it crumble. Wouldn’t that be something
https://alexberenson.substack.com/p/urgent-stunning-data-from-south-africa
"In 2021, Berenson tweeted that COVID-19 vaccinations had led to 50 times more adverse effects than flu vaccine. PolitiFact rated the claim 'mostly false'.[6] The Atlantic called him 'The pandemic's wrongest man', owing to his false claims of the vaccine's ineffectiveness."
https://en.wikipedia.org/wiki/Alex_Berenson#COVID-19_pandemic
Thank you for sharing. Given I have no final formed “opinion” I tend to read many different ones..I already know the general narrative given by the government in coordination with various agencies and mainstream media. Since I cannot make snap judgments based on any opinion or theory—this crisis has been difficult to decipher because it is not binary having been caused by typical oversimplification of a subject. Even though it is happening.
So there seems to be an area of blending between the virtual world and the natural world. Like a hurricane that hit one area became every area even though the sky was sunny where you live. So the known became a belief that is ungrounded. Not empirical practically speaking. Data then if data is all we possess can be quantum and the quantifier’s view is not necessarily fact but becomes fact if believed. Yet the fact is not located in physicality because the presupposition that data is proof of fact is quantum-ly strange in a truly tantum scenario. Simply- location implies empirical fact giving data it’s useful purpose but not a universal one. In situations such as these..We must rely as humans on narrative—and our experience. But is that anecdote? Anecdote cannot necessarily be antidote because again what is the reality or philosophical governance believed by the “reporter”. I constantly recheck my own presuppositions especially as discrete facts alone become more and more nano. In our world the only Absolute is change whereas great faith is being required to accept the unseen. This causes a scientific religiosity in a community that once was driven more materialistically. Now it has become somewhat gnostic. Scientific Gnosticism. A separation between the body and the mind. The virus being an evil archon and the scientists some, the high priests of secret indecipherable knowledge.
There exists, a large reductionism to sift through for a simple person such as me. High complexity abiding only in data that is presupposed to be physical proof leaves an outcome that branches in multiple directions-and that is how the data “feels” both fractal and ouroborean if you could take a snapshot. And the template begins to look more and more like chaos which if consciously viewed as template looks like the collapse of everything. Such as when a pebble hits a windshield and gradually….well you know the rest. Misapplication of one size fits all..has resulted in chaos..
The hurricane is caused by data and undifferentiated emotion which tessellates seemingly infinitely in a bounded space.
Quite agree with your “this crisis has been difficult to decipher because ... typical oversimplification of a subject”. I came over here because of several comments by AlmostWrong on a Substack post by Alexandros Marinos on Scott Alexander’s “take-down” of the ivermectin studies posted by Ivmmeta:
https://doyourownresearch.substack.com/p/a-conflict-of-blurred-visions
AlmostWrong is certainly a prolific writer who imparts a lot of detailed statistics, most of which I really don’t follow. But I had to question his “Delta variant AY.4.2 is spreading even better in the vaccinated than unvaccinated.” Not sure what the source for that claim might be but offhand it seems that that might be due to the way the data is obtained. Maybe – I emphasize the term, maybe – there are more cases among the vaccinated than the unvaxxed simply because there are more of the former than the latter. Or maybe the vaxxed are more likely to get tested than the unvaxxed.
But regardless of how accurate that specific scenario may be, it seems that part of the problem is that the statistical data is probably subject to any number of confounding factors that are not at all easily quantified. And part of that problem may be that there’s no model of the mechanisms involved – something that Marinos touched on if rather briefly; that there’s no understanding of how ivermectin might contribute to the differences in the results over the more credible studies. Absent such models – apart from “worms!” – it seems rather difficult to determine if the statistical results make sense, are credible. As bad as doing phrenology without any model how different psychological traits might affect skull bumps and hollows.
Which is unfortunate as there is in fact some decent models available that may give an inkling of what’s “happening under the hood”. For instance, this NCBI article below shows that Ivermectin does, in fact, have some anti-viral effects. But those come from the fact that its target is "not a viral component, but a host protein important in intracellular transport". Entirely different chemistry from the Pfizer & Merck anti-virals under development.
But that kinda makes ivermectin somewhat toxic at the "half maximal inhibitory concentration" (IC50) level, and not particularly effective at the "highest regulatory approved dose of ivermectin" which is at least a thirtieth to a fiftieth less than that IC50:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7172803/
However, as the article suggests, even at that much reduced level, it may be "key to enabling the body's immune system to begin to mount the full antiviral response before the infection takes control." And that benefit may well contribute to *some* of the differences in the Ivmmeta studies - even apart from the effects of possible worm infections.
But those benefits look to be marginal at best - entirely consistent with the concentration levels of recommended doses - and likely to manifest themselves to any great or noticeable degree only when the patient was more or less on death's doorstep. Which seems to describe many of the Ivmmeta tests in question.
Would be interesting to try creating a patient model that incorporates those effects to determine if they would be sufficient to explain many of the Ivmmeta test results.
"who imparts a lot of detailed statistics, most of which I really don’t follow."
I have to say I'm sorry I do a bad job of writing. If I am wrong, it makes my wrongness not spread far and wide due to poor presentation, which is a relief.
On the other hand, if I am right, I was hoping someone more intelligent, skilled or influential can piece things together and make it usable. Apparently that's not yet happened, and it could be because I'm not able to make my case and that my case is not right.
As for AY.4.2 spreading (like omicron or any variant), the odds of being infected with a variant of the dominant strain is higher for those who have had some prior exposure some version of the dominant strain. In the case of vaccination, there is acute exposure to the spike protein in most vaccines and whole virus in others. The reason why a variant spreads faster (shows increasing incidence) in vaccinated vs unvaccinated is because unvaccinated either have no exposure to the virus or have exposure to slightly different mutants of the virus. When a mutant want to spread, it has to make no adjustments when it faces successive hosts with a cloned vaccinated immune response [as it's been programmed to neutralize wuhan virus]. It cannot easily do this for unvaccinated because unvaccinated and uninfected have innate immune response that neutralize all variants except those which are more transmissible, and unvaccinated recovered all have seen some version of the prevailing mutants making them harder to re-infect. This leaves only the vaccinated vulnerable. What I tried to show is that the 12% advantage that AY.4.2 had in spreading in vaccinated was after adjusting for confounders and testing and that the real reason why it was spreading is because young children at schools who were exposed got vaccinated, caught the virus and then infected their parents while this didn't happen for unvaccinated because the viruses they got infected with were all slightly different from each other and hence added up to nothing in terms of dominance.
Dear AlmostWrong. I spent some time this pm reading your comments to others. It confirmed what I saw in you if seeing can be attributed to reading. While I work on a response to Steersman here is what I wrote:
Well, AlmostWrong impresses my simple mind because I though ignorant, discern in this work, that, AW does not presuppose, rather asks instead the questions which precede answers that require “asking before proceeding.” AW’s ego which is merely an adaptive acquired mechanism does not fully override his/her heart and natural will for health for others.
Dear Robin, I look forward to reading your replies and the resources you share. The will to learn and self-correct is strong because as your correctly sensed- I want nothing but better health for all without sacrificing anything in the process we collectively hold dear, rather strengthening and improving our reliance tools that will not sabotage our own abilities to make amends if this over and critically so if this is not over, and just the beginning.
“I have to say I'm sorry I do a bad job of writing.”
Doesn’t seem all that bad.🙂 Though I can sympathize – I’ve written and posted a number of articles thither and yon – Medium, The Post Millennial, various blogs, etc – and know how difficult it can be to put words to paper in a coherent and readable form. “Writing: Craft & Art” by Rivers gave me some pointers that you might look into, though there are many other such sources.
And a couple of times I’ve even contracted a professional editor for assistance, though that can get a bit expensive. In any case, the latest was for this essay on Wikipedia’s Lysenkoism that you might have some interest in:
https://medium.com/@steersmann/wikipedias-lysenkoism-410901a22da2
Big fan of Wikipedia in general, but when it comes to sex and gender, their vaunted “neutral point of view” is in tatters.
“the odds of being infected with a variant of the dominant strain is higher for those who have had some prior exposure some version of the dominant strain”
That may well be the case, but I wonder if you have any sources from biological or medical sources that would justify that argument. Seems to me that if the statistical results are not consistent with the models of the underlying process then either the model is inaccurate and there are other processes and factors in play, or the statistical sampling and the inferences drawn from it are flawed.
Partly why I alluded to Marinos’ reference to mechanisms, the NCBI article on ivermectin blood concentration levels, and “worms”, all as relevant models that may have some bearing on the results of those Ivmmeta studies. Something that you with your “physics training” should appreciate. 🙂
Thank you for the tips. I will try my best to incorporate and look forward to reading your article. I'm poorly trained in Physics I must say, but I will promise you this, I will write a detailed article explaining everything but that I was hesitant because as I mention in other comments, it's not enough to have models and plausible mechanisms, what we need is raw data that satisfies equations not merely directionally (that is it's not important be to just right about whether the effect statistical or mechanistic exists in the direction specified) but also in calculable size. Put differently, it's not sufficient to show "worms" or "co-infections" prevalence and ivermectin use might free off resources to fight other infections, but to actually precisely define that if this were not the case then what we would see. In the case of ivermectin, if the utility is limited to indirect benefits of intestinal infections then we should be able to say with confidence that ivermectin will not be able to clear infections of other kinds. This allows us to produce counter-factual which can then be used to invalidate the exclusivity of mechanisms. For example: Here you can see ivermectin was used to cure a urinary tract infection in a chronically infected covid patient at day 56 of infection to day 60. The infection resolved but covid did not. https://www.nature.com/articles/s41467-021-26602-3/figures/1
In my case, before I make my case more clearly that will take much longer as I gather the empirical data to be 100% sure of what I am saying, I had to put out this information in a haphazard way so that I can clear up my conscience that I didn't wait too long and allowed perfect to be the enemy of good enough. Therefore, I've put out this information, I will explain it properly as I gather more data specifically reinfection by vaccination date and once I have that, I will be able to prove or disprove conclusively what I think is happening.
Out of desperation, I appealed to UKHSA to release this data here:
https://almostwrong.substack.com/p/request-boost-reinfection-data-classification
Next I will ask Danish Authorities in the next day or two after I have collected more data about reinfection prevalence.
Sorry for not being able to make my case, but if I am wrong, no problem. If I am right, I needed to get this information out as soon as I could so that other people who also understand what I am thinking can take action.
I read your comments at Dr. Vanden Bossche’s substack. Something below that I read which seems Almost Right for Almost wrong to think about😊.
Thank you!~ It's very intriguing that China is by all appearances and actions, the last bastion still standing against Covid-19. Also intriguing that they were the first country where it broke out as well. Lot's of unexplained and undetermined observations. Will it crumble?
Will it crumble? China has the same big problems the rest of the world has….with a lot less water…but frankly? Dunno.
Anyway…
It’s a strong paper by Ethical Skeptic who I follow periodically. IMHO I think he proves his point(s) but it requires on my part a complete recalibration of the whole narrative or at least large portions of it. So the rest of the world followed China’s example using authoritarian measures based on error filled presuppositions. The timeline and transmission matter. I get that.
I notice however that Ethical Skeptic completely left out the MIC involvement with China in the “shared” research as noted in Ralph Baric’s correspondence records. Given ES was in Naval Intelligence I always look for omissions like that too.
Oh what a tangled web.
https://theethicalskeptic.com/2021/11/15/chinas-ccp-concealed-sars-cov-2-presence-in-china-as-far-back-as-march-2018/