
What if the Negative 10.5% Vaccine Effectiveness explained the AY.4.2 Delta Plus ~10% Transmissibility Advantage causing an outbreak?
Only to be replaced by something worse.

(Edit: Only a draft idea will write a proper article with citations and credits at some point)

Shortest TLDR Attempt: Delta Plus AY.4.2 Strain transmissibility is a temporal artifact of age-stratified progressive mass immunization strategy, with vaccines that upon first exposure in those already infected, enhance the acquisition of infection and/or result in precipitation of the disease.
Transmissibility advantage is only within the framework of a host population-virus interaction setting (Congregate + Household), that is conducive for spread due to high background infection rates, prolonged segregation, self-similarity or lack of heterogeneity in the host immune status and lack of exposure to competing pathogens.
It will dissipate the moment infection prevention measures are relaxed, age based mass immunization strategy changed, or quarantine measures for new vaccinees are introduced after virologic/serologic screening, or congregate settings sterilized (impossible with virus replication favorable indoors air properties and no UV sterilization), or entire population from ages 0 to 100 universally vaccinated on the same day and then vaccinated again as soon as possible with the second dose.






Caution: if we continue with our current interventions, we will lose more lives in the older population as has happened in Ontario and is happening in other care homes as we speak. Delta Plus will almost certainly more lethal in the Hospital and Care settings where mobility of people is low.
Working Draft [Caution, I’m not a writer, so if you wish to help, then please correct my form, grammar or composition. But most important, correct my reasoning or assumptions if wrong or unconvincing. Re-use or re-label anything. Just want to get the word out. Will cite sources and give credit for the visualization before final draft. I’m just trying to add anything fast that I can to this slow unfolding nightmare]
TLDR Longer Version:
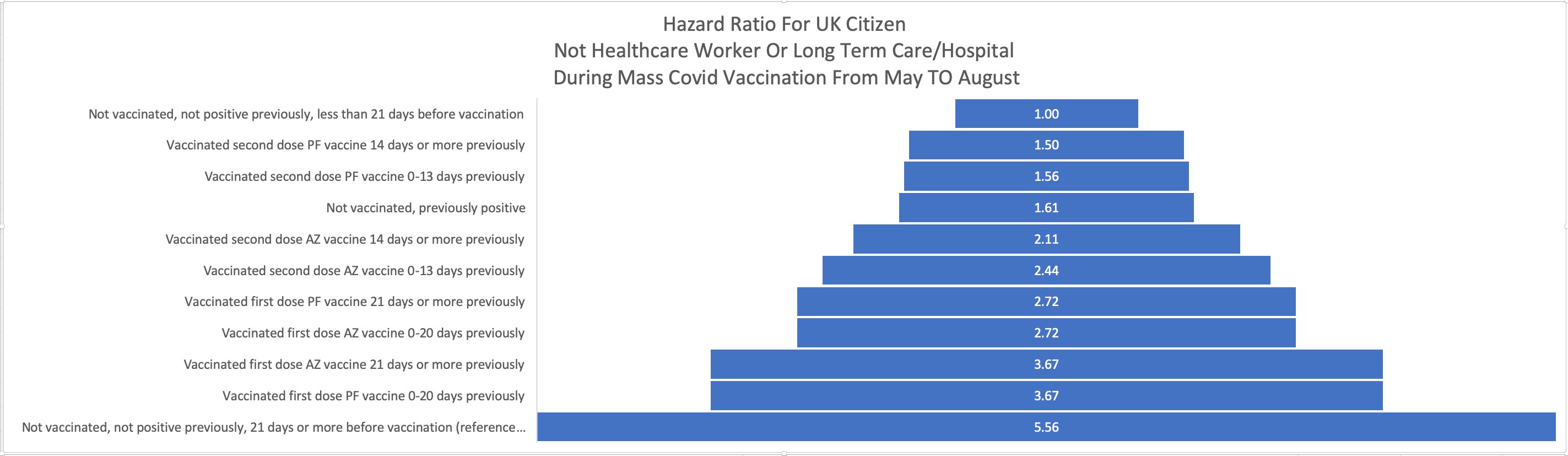
Pfizer’s Safety data Filing from June is not inconsistent with my theory that Asymptomatically infected persons upon first Pfizer vaccine exposure will contract infection at rate 10.5% higher than placebo. And likely much higher than the risk averse general population who wouldn’t sign up for experimental trials at all.
Therefore, repeated Vaccine Exposures will increase the prevalence of SARS-COV-2 Virus at the rate of 1.1x as many SARS-COV-2 Carriers get vaccinated.
Increased prevalence improves willingness of new vaccine exposures while it increases simultaneously their likelihood of being infected while they are receiving the first exposure to the vaccine product.
This will result in an outbreak where the most transmissible variants will be ones the vaccinees shed and simultaneously become susceptible to.
When the unvaccinated and people vaccinated long time ago have been infected, the outbreak ends until the virus finds new cohort of vaccinees to infect (For example: Children 5-11)
The advantage is conferred by the sudden change in the Innate Immune status of the recipient, not anything intrinsic about the virus.
When vaccinations stop or end, and the vaccinees mix with non-vaccinees, the advantage will dissipate quickly as it faces competition.
Alternative solution is to not vaccinate immunocompetent hosts who are likely to be carrying a benign variant which will be undetectable until they are vaccinated and a virulent less sensitive strain attacks their body.
Testing people for the (prior) or current infection as a condition before vaccination can reduce the size of the outbreak but cannot eliminate it.
This is because prevalence during vaccination is unlikely to be low. The willingness of at risk to be vaccinated is high. The prevalence of new infections amongst those who are deemed to be at risk is also higher each round of vaccination. So the outbreak is inevitable with this kind of leaky vaccine that increases susceptibility by clearing the body of benign sensitive variants and giving competitive advantage to variants resistant to the vaccine.
Only condition where screening can prevent can outbreak with this kind of vaccine is having no SARS-COV-2 infections in the past x days and x mile radius when the first vaccinee is exposed and then they are immediately quarantined for as along as they cannot get their second dose. In this time, no new infections can happen. If the vaccinee was carrying a latent infection or was newly infected, the vaccine will precipitate into COVID-19 case a few times. At this time, only recovered or recently fully vaccinated healthcare professionals should treat the vaccinee as they are likely to require hospital care. Newly vaccinated, unvaccinated and vaccinated long time ago are at great risk of new infection and should not interact with the vaccinee. This is the only way.
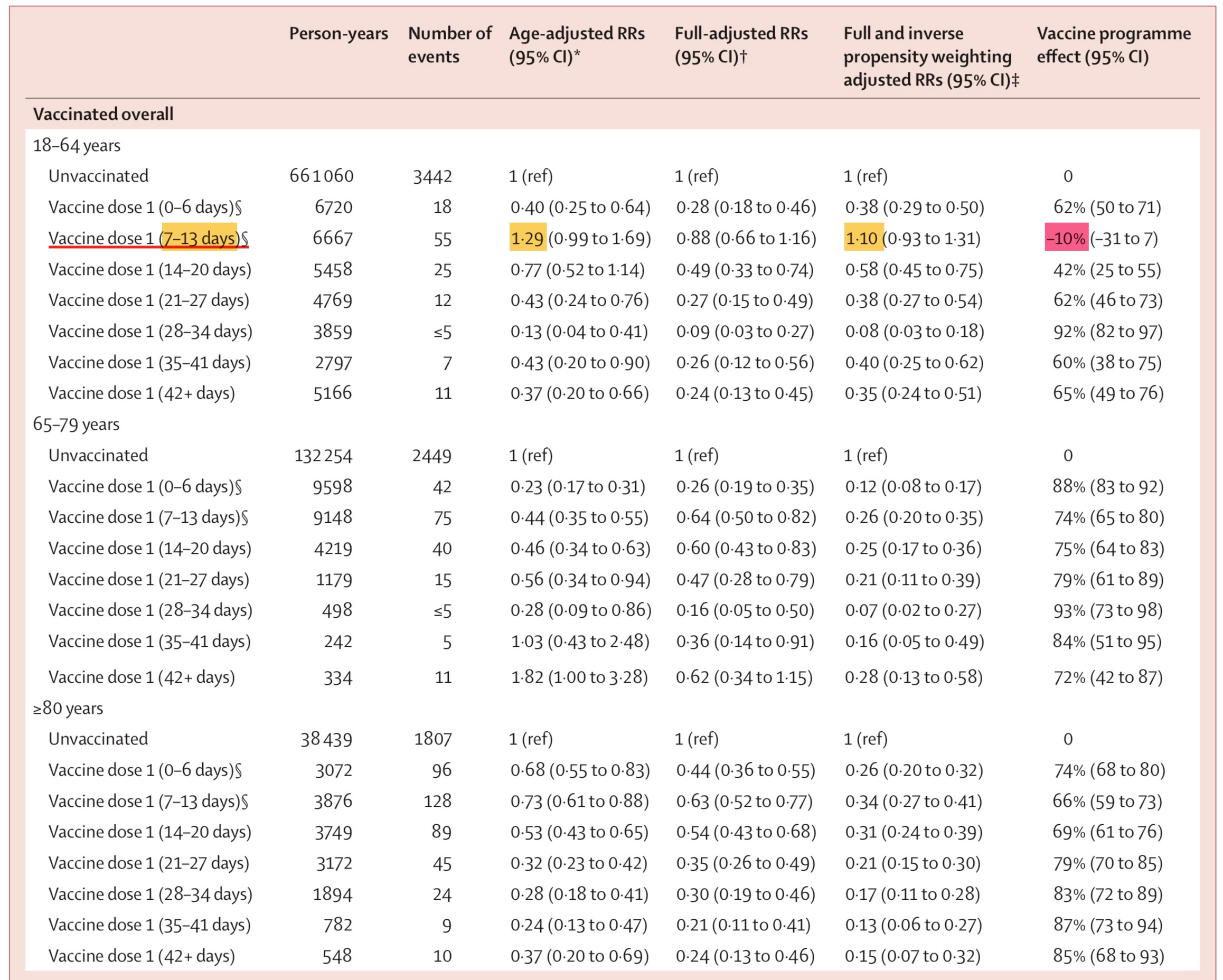
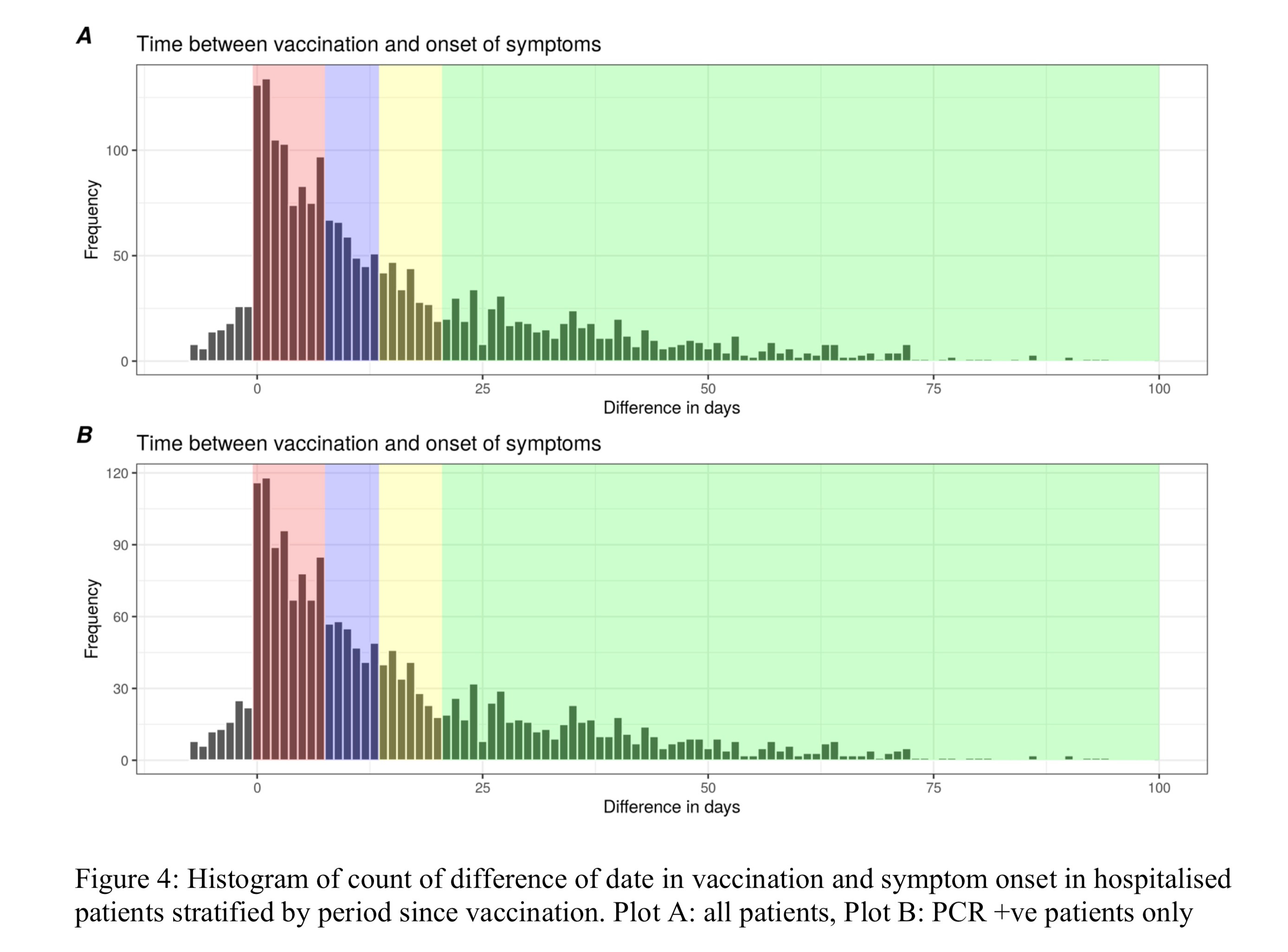
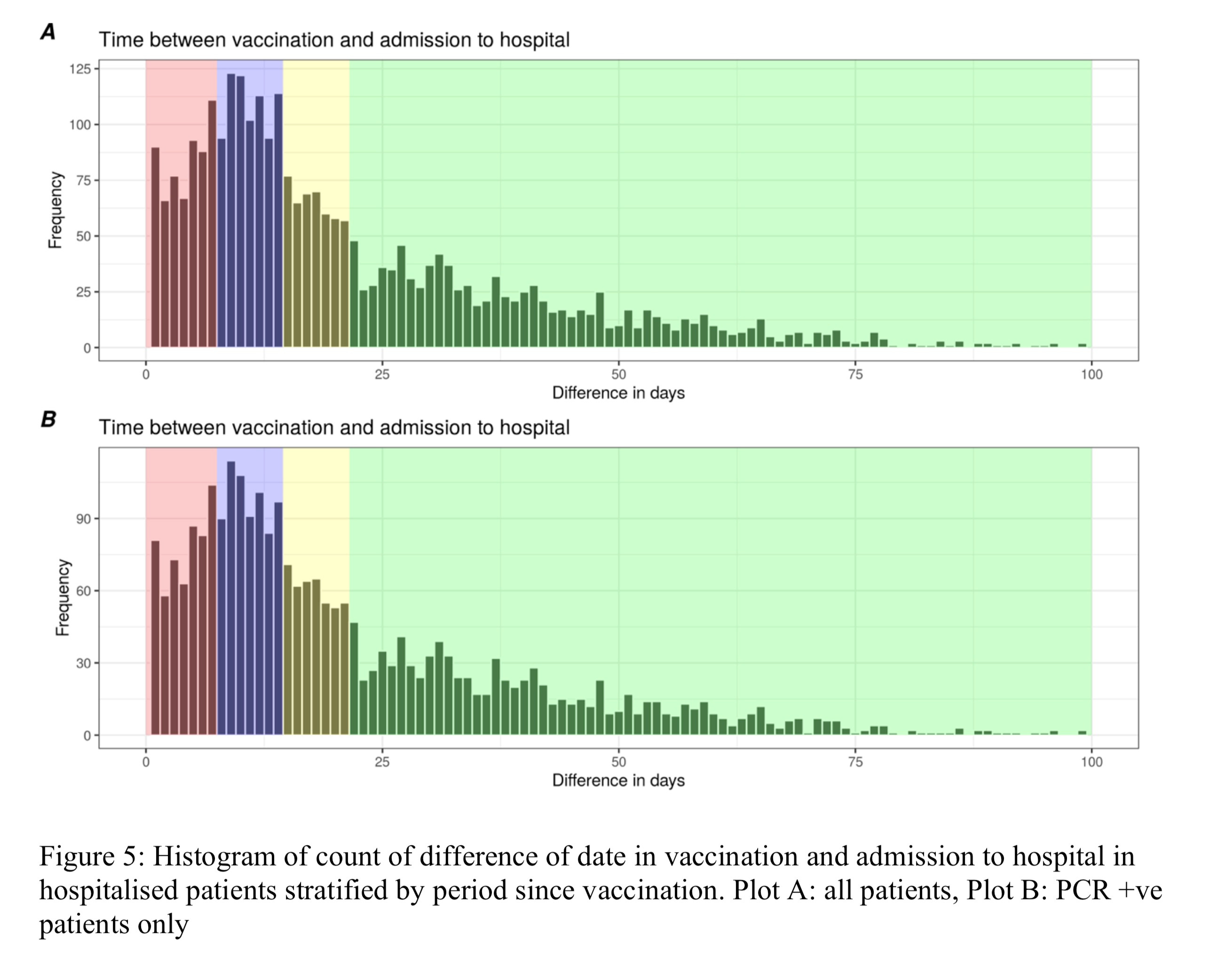
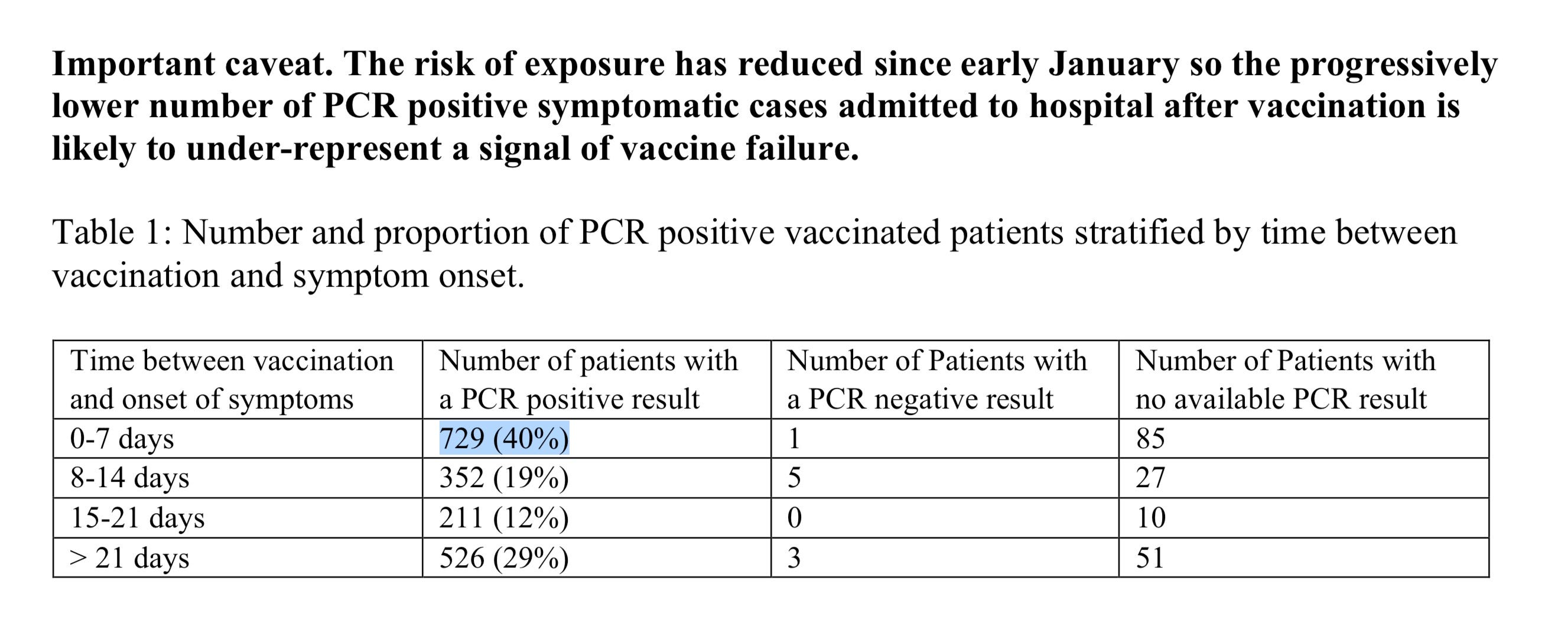
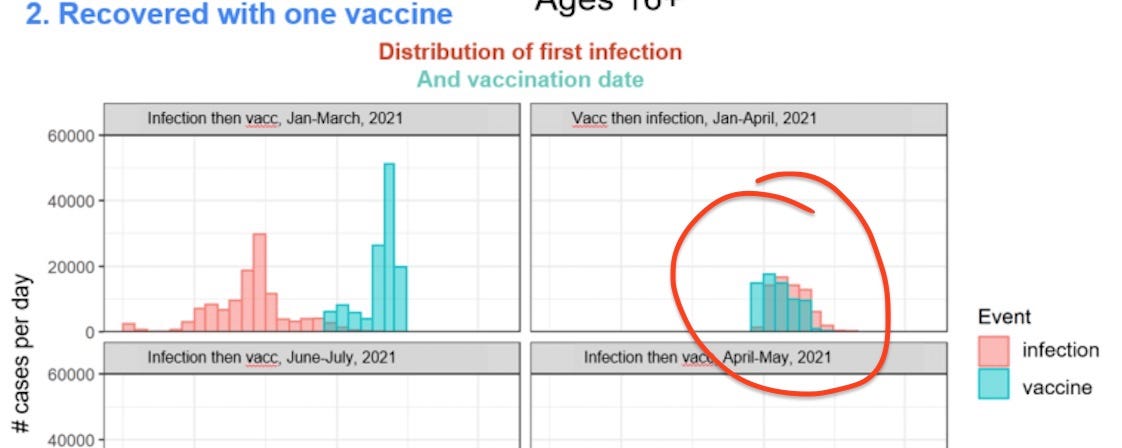
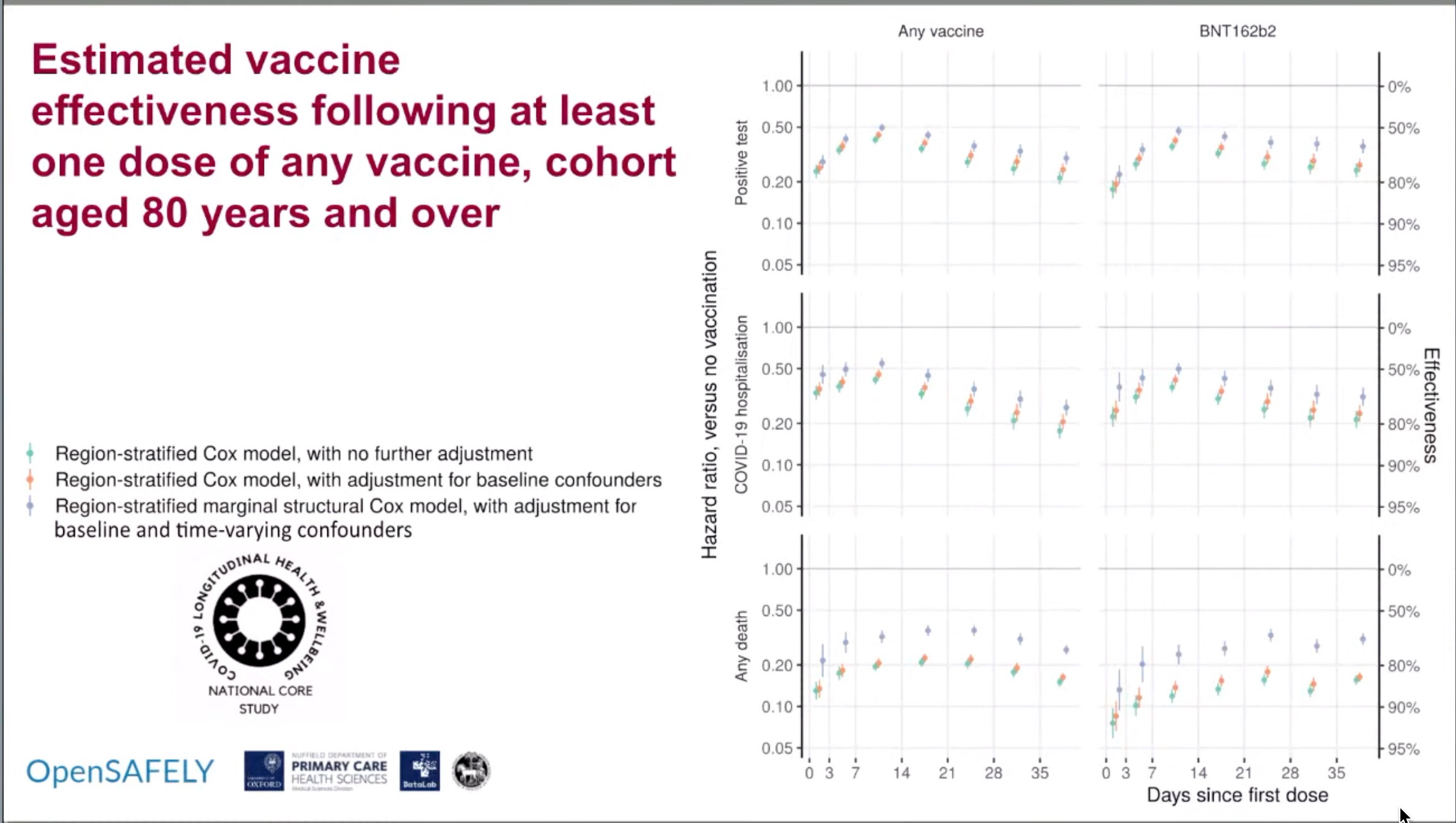
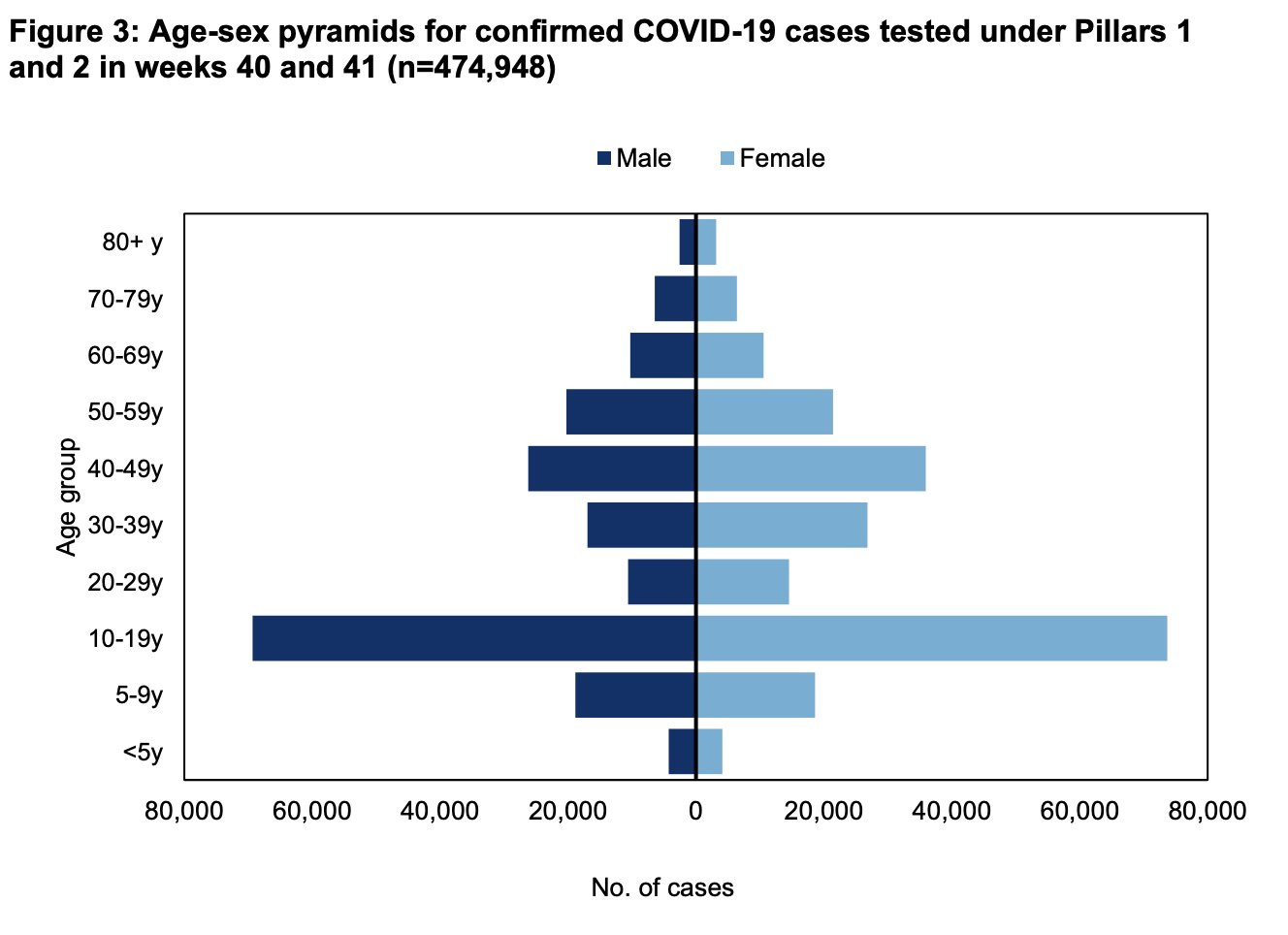
a. UK presenting infections/deaths after 1 dose of vaccine and admitting that the more immunogenic Pfizer vaccine is also elevating the risk even higher for infection compared to Astrazeneca
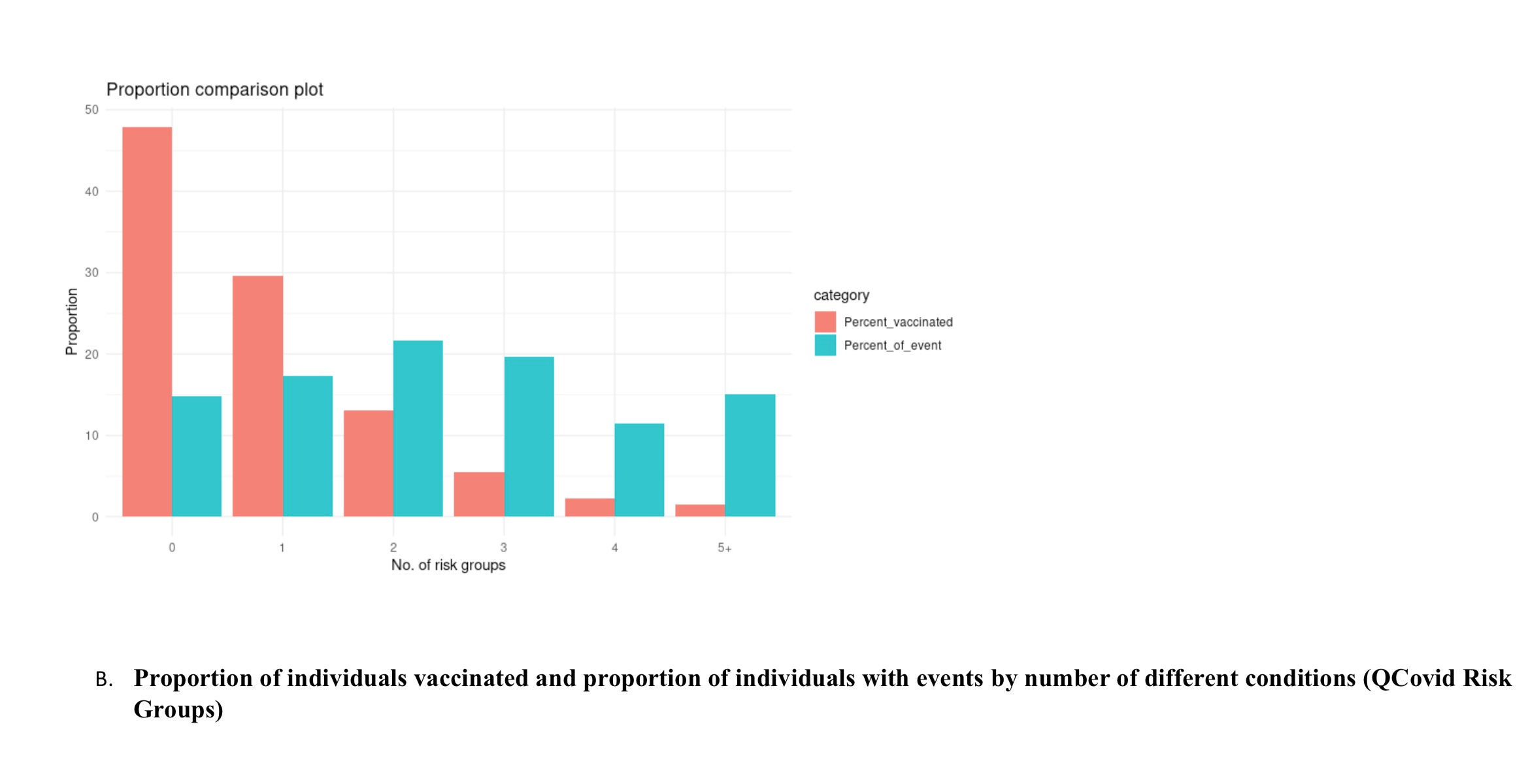
"We observed an abundance of patients admitted to hospital within 7 days of vaccination (Figure 3)."

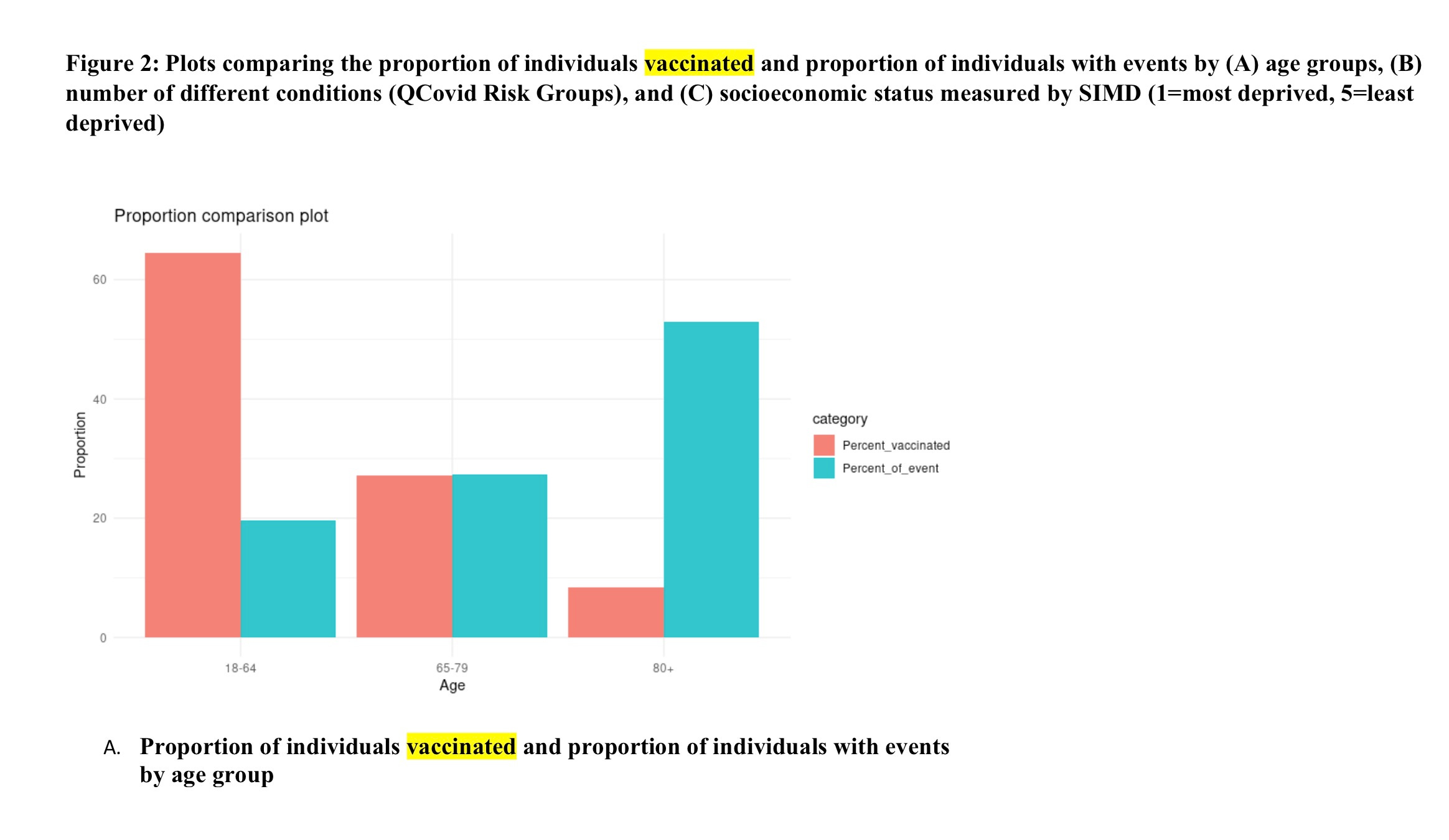
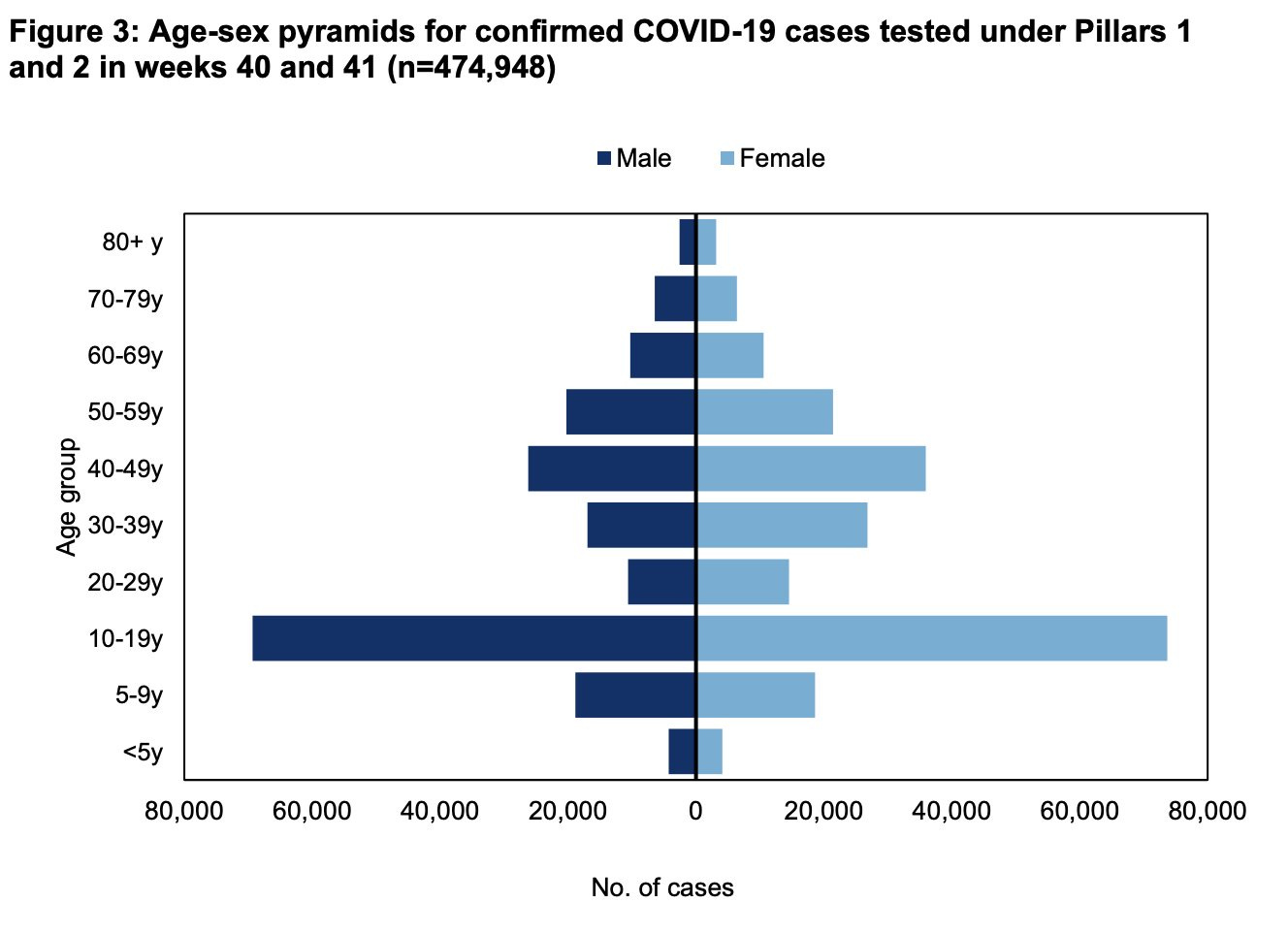
"Figure 2: Infection following vaccination shows a non-linear relationship with age, with risk increasing particularly in adults aged under 40 years"






Denmark Infections 



Longer Version: [Still Writing, ✍️ Editing, etc. ]
First. Read These Threads by Prof. Francis Balloux or @kallmemeg To Catch up.





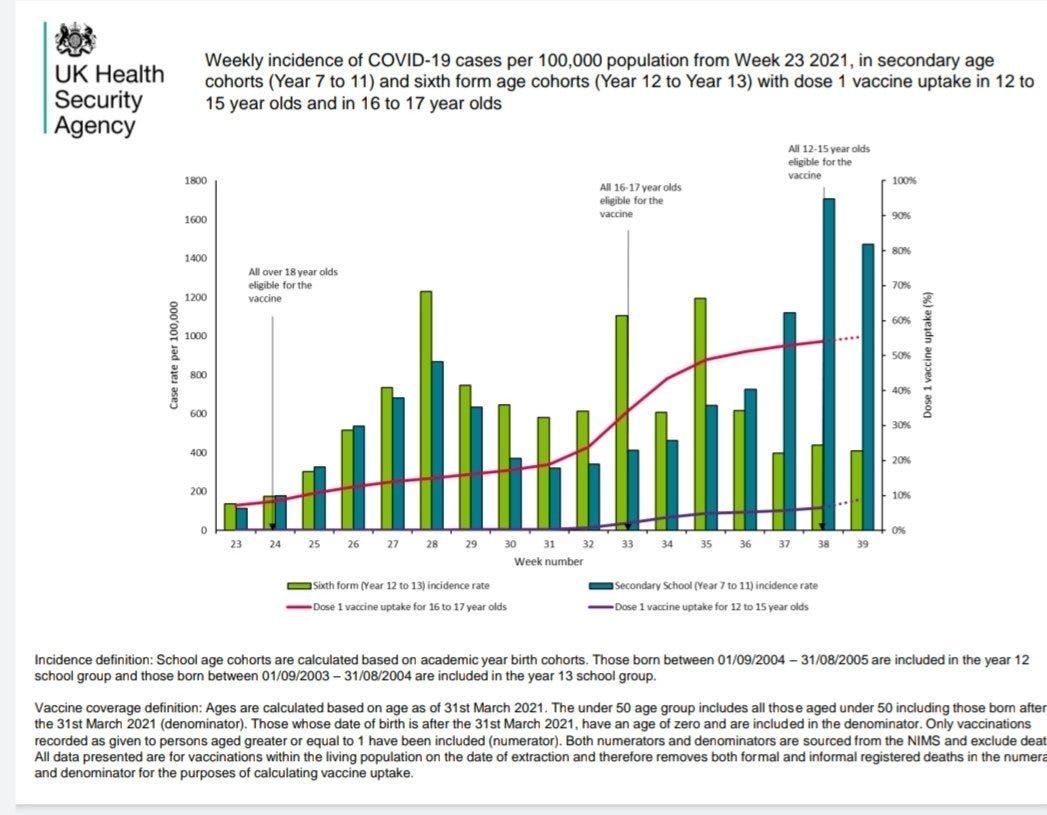
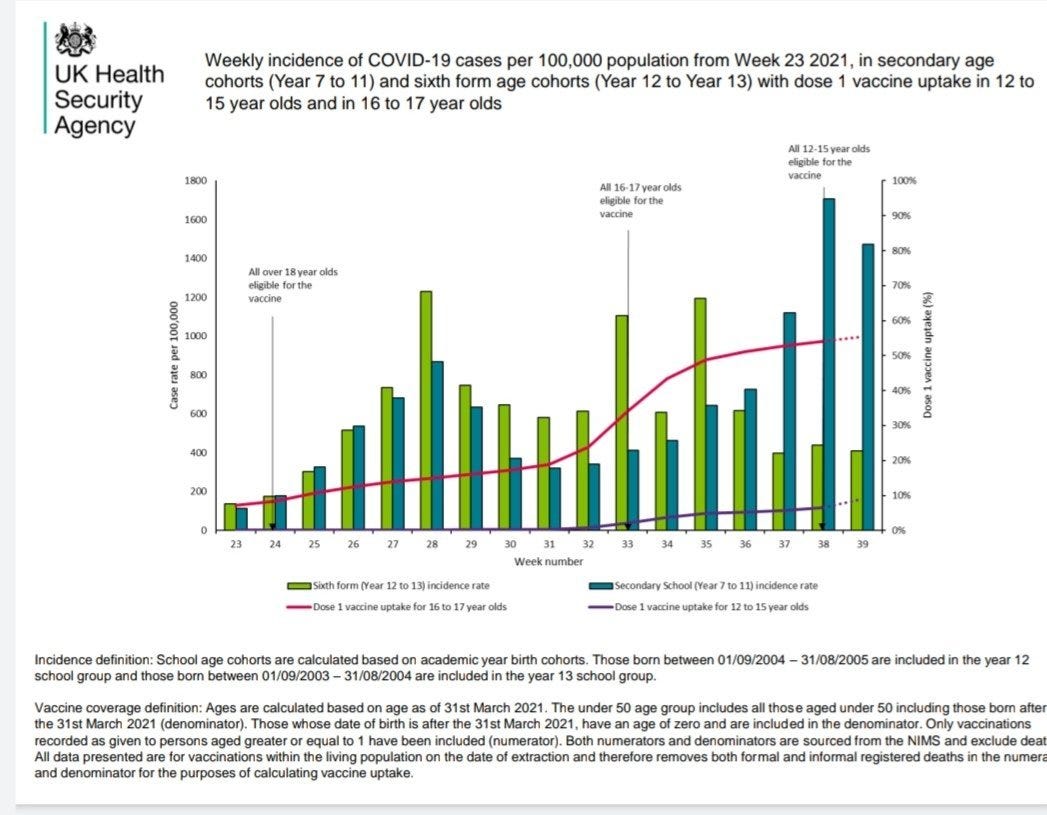
Summary: A New Delta Variant has been spreading and replacing the original strain steadily since Week 34 in the UK (week 32 if you consider the 14 day delay from sample submission to graphed point). It’s estimated based on the rate of replacement that the inherent transmission advantage is ~10-12%.
This is based on the belief that if something is not region specific (and the variant is spreading everywhere in the UK) the change is not due to some kind of founder effect. That is, you expect something to grow locally if it has a local source that’s seeded a huge outbreak.
But is that kind of analysis enough?
Of course not, because the data is not controlled for *Intervention* specificity. We cannot assume that just because something is happening independently in different regions, that it doesn’t have a common specific intervention associated with it.
In fact, the data is not controlled for the two most important factors because we all know if they tried to control for that, it might reveal something very unpleasant. Age and Vaccine Exposure. The UK Variants of Concern report explicitly
Why is Age and Vaccine Exposure Relevant?
Because the national Mass Immunization programs can shift the disease burden in ways that’s highly modulated by the timing, fraction and homogeneity of uptake during an outbreak. India, Denmark and UK all followed the same strategy of carefully vaccinating by Risk group, then Age group, pushing nosocomial infectious transmission pressure onto patients, care home residents and then their children (who were young or Middle Aged adults).
In India, this took the deadliest turn in the entire pandemic due to high chemoprophylaxis + whole virion/spike protein vaccinal exposure selecting highly virulent and transmissible strains that resulted in primarily enteric forms of the disease followed by viremia and shortness of breath. Remdesivir abuse had made that treatment worse than worthless by that time. Something that didn’t happen with the original strains where the disease was much more associated with inflammatory responses. The original virus wasn’t causing healthy young people to be short of breath and on oxygen. The young people who died in India died due to unchecked replication and hypoxia. The origin was likely reservoirs in out own body from previous infections. Even though Singapore says Mild cases, the number of people on oxygen. The next deadly strain is likely to come from places like Israel or Singapore: Merck Drug (Upping Mutation Rate, Killing Fragile Hosts due to Toxicity, Immunocompetents who survive the toxicity will select for virulence) + Delta Specific Vaccine (Selecting for ) + 100% vaccine uptake.
Still Working on Draft Thoughts.
Stop Universal Vaccination
Mass Vaccination during high viral prevalence will allow adaptation
If you must Mass Vaccinate,
then quarantine Vaccinees from their peers and parents
Do something scientific about the dosing protocol. Applying a uniform amount on pressure when the fragility is highly variable will lead to a situation where the variants will be resistant and the vaccine will be toxic to children. We will kill both, Adult Population with highly virulent strains that competed and won easily against sub-optimal vaccine doses and hyper-competent immune hosts who were overwhelmed with virus all around. or the Children through high toxicity of drugs needed to prevent and treat infection. This is a lose-lose if we are not being empirical.
Oral vaccines/Nasal Vaccines For Under Fives. Need Sterilizing Immunity without transmission.
Heterogeneity is not our enemy, it’s a strength but forcefully introducing homogeneity might work better or it might be unleashing hell. The problem is the irreversibility of certain medical interventions. So we should be careful about reducing host diversity because we may no longer be able to use mixing as a form of infection control measure when everyone is equally immune or equally susceptible. SARS-COV-2 is formidable, but it’s not highly adapted yet to Humans like Rhinovirus. Infection control measures reduces competition and ensures viral evolution for SARS-COV-2. If you were infected with Rhinovirus and SARS-COV-2, Rhinovirus outcompetes in viral growth and enables a complete immune response that also clears SARS-COV-2.