UKHSA Reinfection Data being requested here might be critical for understanding trends. trends they may not anticipate, but many of us might be fully aware. If you can show interest in this data stratification, it will help me and others a whole lot trying to understand and predict what’s coming next.
Please show your interest in this data now if you believe the raw data will be useful for future generations to figure out what happened in 2021 before it’s written out of history or erased from the hard disks with bleach bit and then presented as an aggregate without order of events and incidence rates before and after our mass interventions.
Updated for clarity on what you could do to help if you agree.
Whose tweet am I being asked to “Like” on twitter?
I’ve linked a tweet by (Igor Chudov) who is requesting the inclusion of a specific category of raw data by vaccine status below.
Why should I express interest in something like this, I don’t want to harass scientists under pressure.
Meaghan Kall is an epidemiologist who works for the UKHSA formerly called the Public Health England. She’s a brilliant, community oriented and feedback responsive researcher that shares UKHSA’s weekly reports on infections. I have the utmost respect for her, and her colleagues at the Agency for withstanding significant pressure and delivering information to not just the UK taxpayer but also everyone else unlucky enough to be living in jurisdictions where this kind of consistency and meticulously collected data is neither collected, nor shared, let alone demanded.
She’s also the focus of people’s ire when the formerly Public Health England’s report started showing worsening vaccine performance implying epidemic danger. She was also recently scolded by “vaccine hesitancy concerned” data representation gatekeepers into removing a very useful infection odds ratio with Delta Plus tableMany of you who follow those reports can appreciate the level of granular detail the reports contain. I do not wish to put additional pressure on an agency that’s frankly under a lot of pressure from the Elected Government, Academics and other interests (including the natural self-interests of those who work for UKHSA and their institutional and personal biases).
Why is this important?
I don’t know that it is important. But i’ve attached a few graphs and spent some paragraphs telling you some of what’s weird and I can’t know why. If it was important, it would be important in bigly way. So, without knowing likelihood of utility, I can still say the effect size is very large for danger, so worth trying even if it’s nothing. Look at the trend here:
I’ve been deplatformed from twitter years now and it’s the first time I’ve asked anyone to ever interact with any thought in two years of the pandemic. This doesn’t mean it’s very consequential for you or me or anyone right now, but it might be, and if it is, this is time we will know it, not 3 weeks from now, not 3 months, not without granular data. We may not be able to understand all of the mechanics but if all goes south from here, maybe future generations will have better access to data to re-analyze the viral spread dynamics.
I’m still skeptical but I would like to keep an eye on this, what can I do?
If you still have access, and do not mind interacting through a “like” only, then please do this one thing that is likely to have the greatest impact in revealing the mechanisms of viral evolution and spread.
If you think you can do this, it will help a lot in verifying many important theories and invalidating others. For example, if UKHSA is correct, the “reinfections before vaccination” group could balloon in the coming weeks. If this doesn’t happen, we will have clear proof that some things are not happening leaving only other possible outcomes which might be good. If we see it ballooning, then we are in for some pain, and stopping it would require significant re-analysis of what we think is driving the pandemic. We spend less time in duplicating work and chasing ghosts. Eliminating worst outcomes fast and quick is one thing thing kind of data can reveal in my opinion that will be obfuscated if presented not as a time series but aggregate “regression model”.
Thank you. 🙏 😊
Remember “reinfections before vaccination” appeared to have extremely high viral loads in the most recent vaccine effectiveness paper from the UK. No explanations were given how they determined “before vaccination” or “re” part.
Okay Done. Now what?
Nothing. Just relax and if you have time to kill or random graphs to eyeball, read further and don’t blame yourself if everything appears random, it’s because I’ve not found the time and space to put it all together but hopefully someone smarter and more capable than I can do it. I’m a terrible writer, and terrible at presentation, and I don’t understand what’s happening, but I am not waiting for people who’ve proven their incompetence at putting us at increased peril to do that job for you or me anymore.
Flashback-December 2020- People surprised that December 7th 2020. the viral load increased in the whole population.
Little Monday plotting sesh, this time ONS infection survey average Ct values (& percentiles) for individuals testing #COVID19 +ve in random sampling
Below, the % of +ve tests by gene for each report week. Clearly see S-dropout proportions, thanks to the new variant, taking over https://t.co/GQcLsMefgt
10:59 PM · Dec 29, 2020
1 Repost · 3 Likes
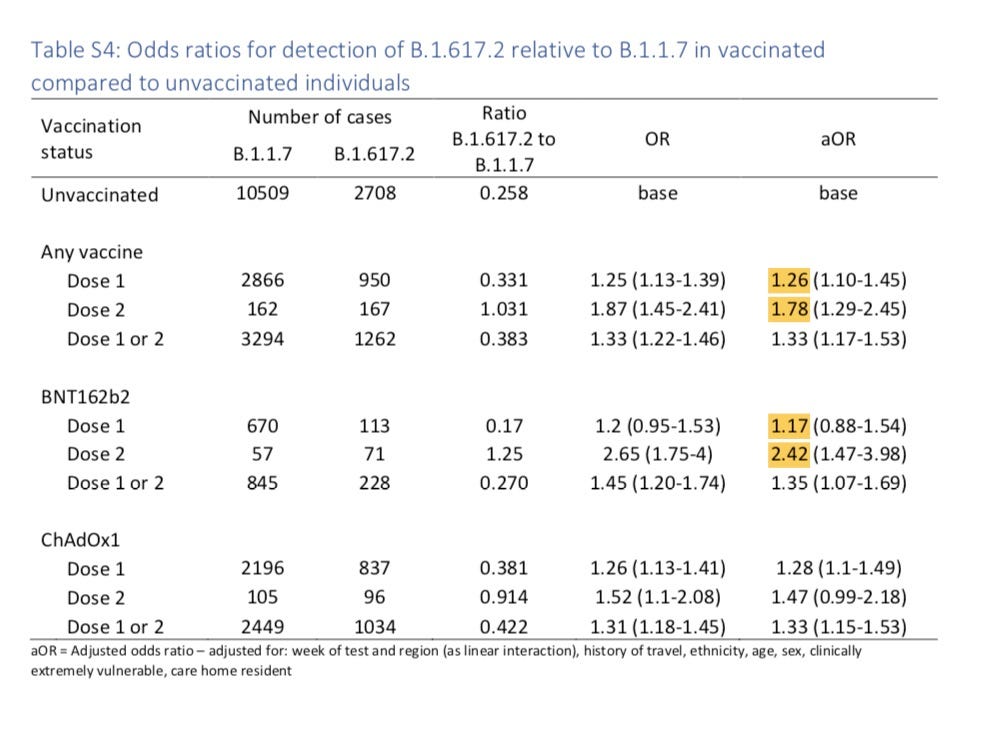
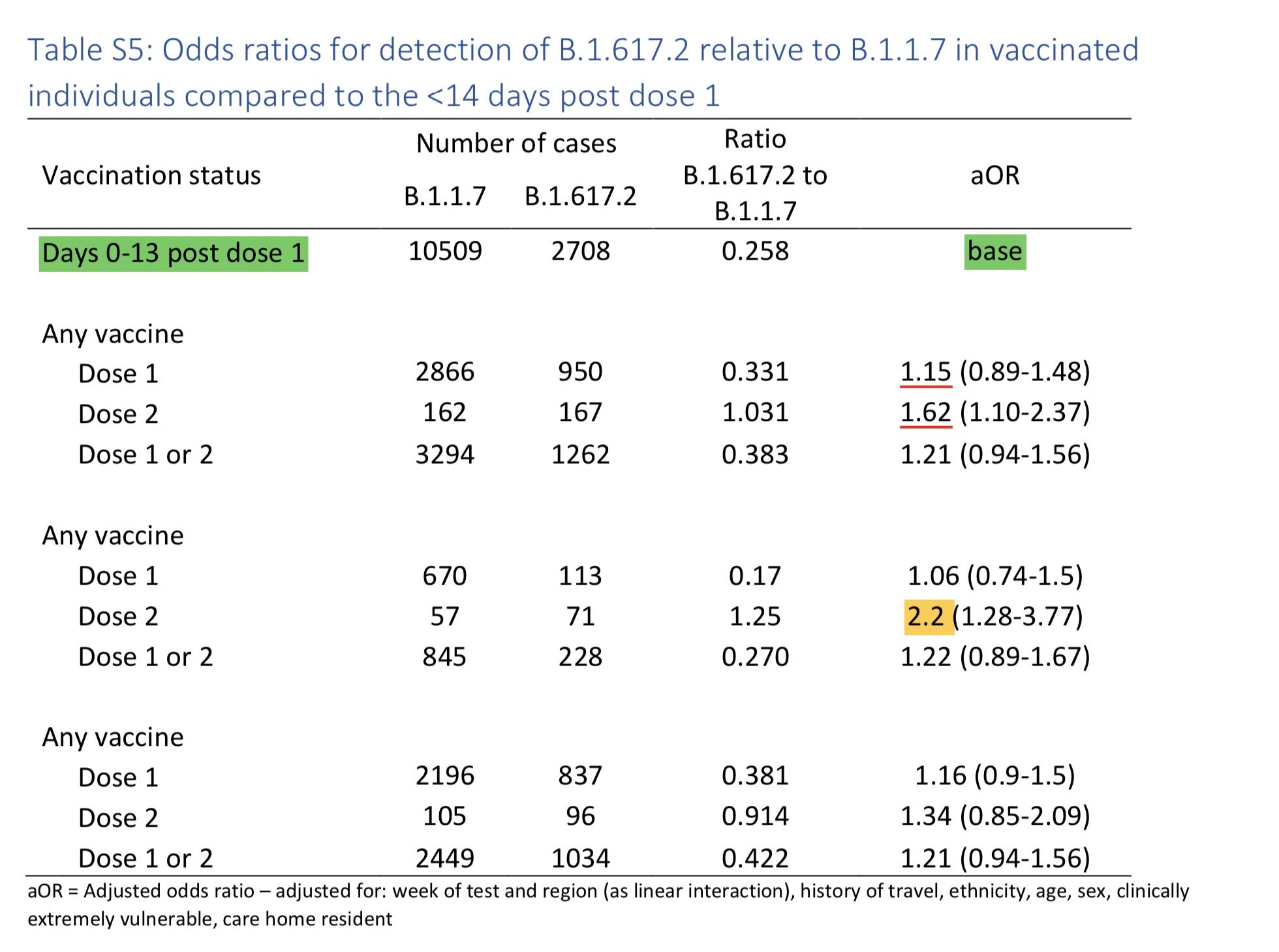
Repeating a few graphs and tables people shouldn’t forget - Vaccinated differentially susceptible to variants not unvaccinated (See 265% greater odds of being Delta infected if Fully Vaccinated from UK in the summer)
Strong purifying selection and enrichment of spike mutants in the population over regular mutants after spike based vaccine prevalence increased.
Check the trend line for “Reinfection before Vaccination” of hyperinflation in viral load.
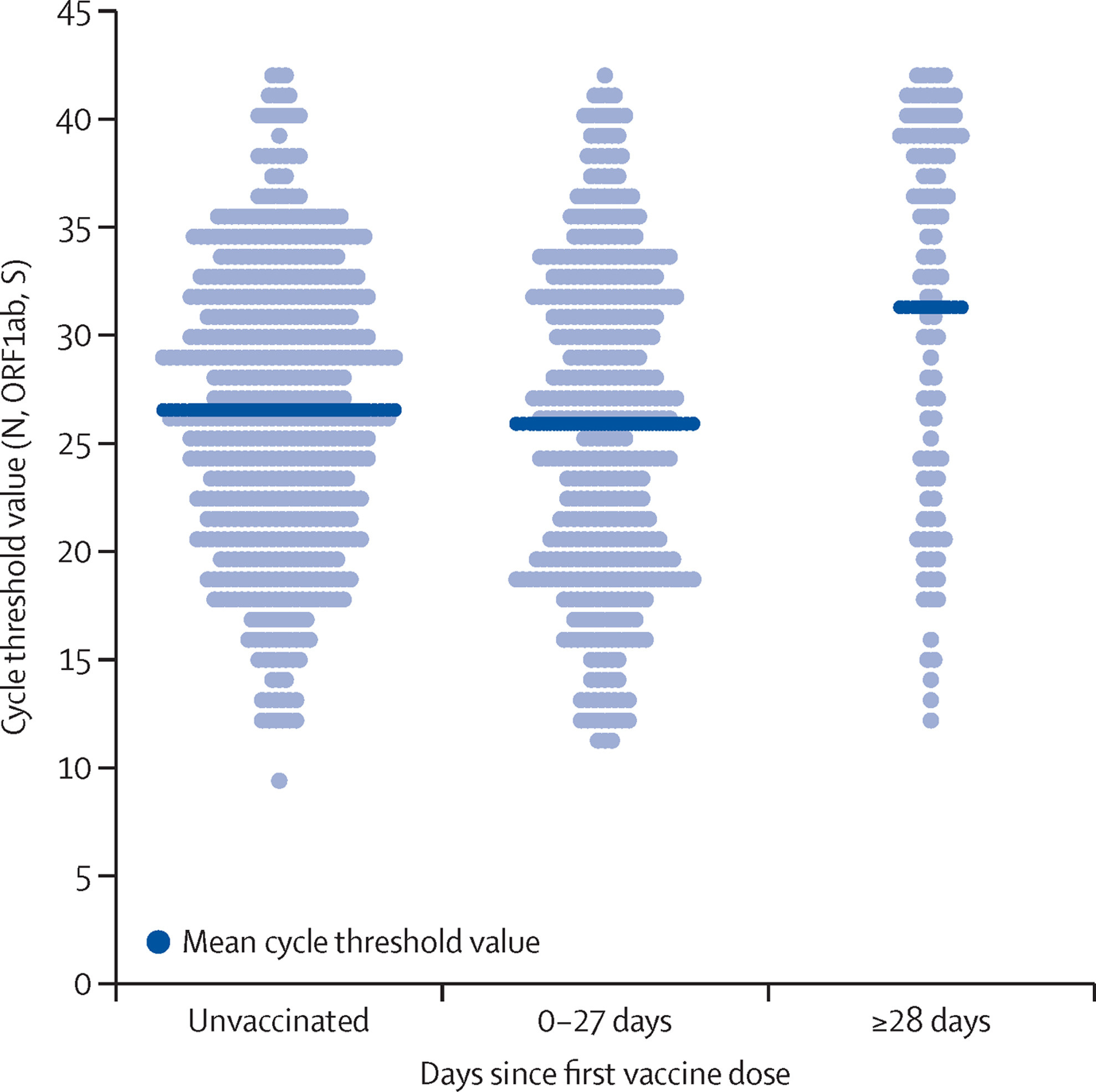
The evolution of this phenomenon started immediately after the first care home residents were vaccinated and got infected in the first days or reactivated viral reservoirs. See viral load in first 14 days in the early days of alpha + delta
You may have heard from many who noticed that susceptibility is higher after the first dose of vaccination for a few weeks.
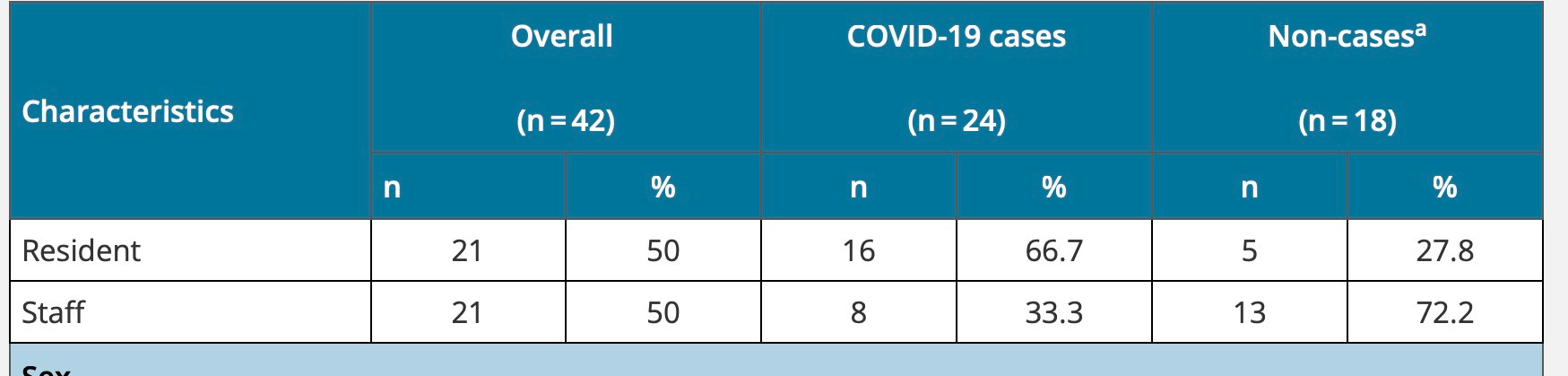
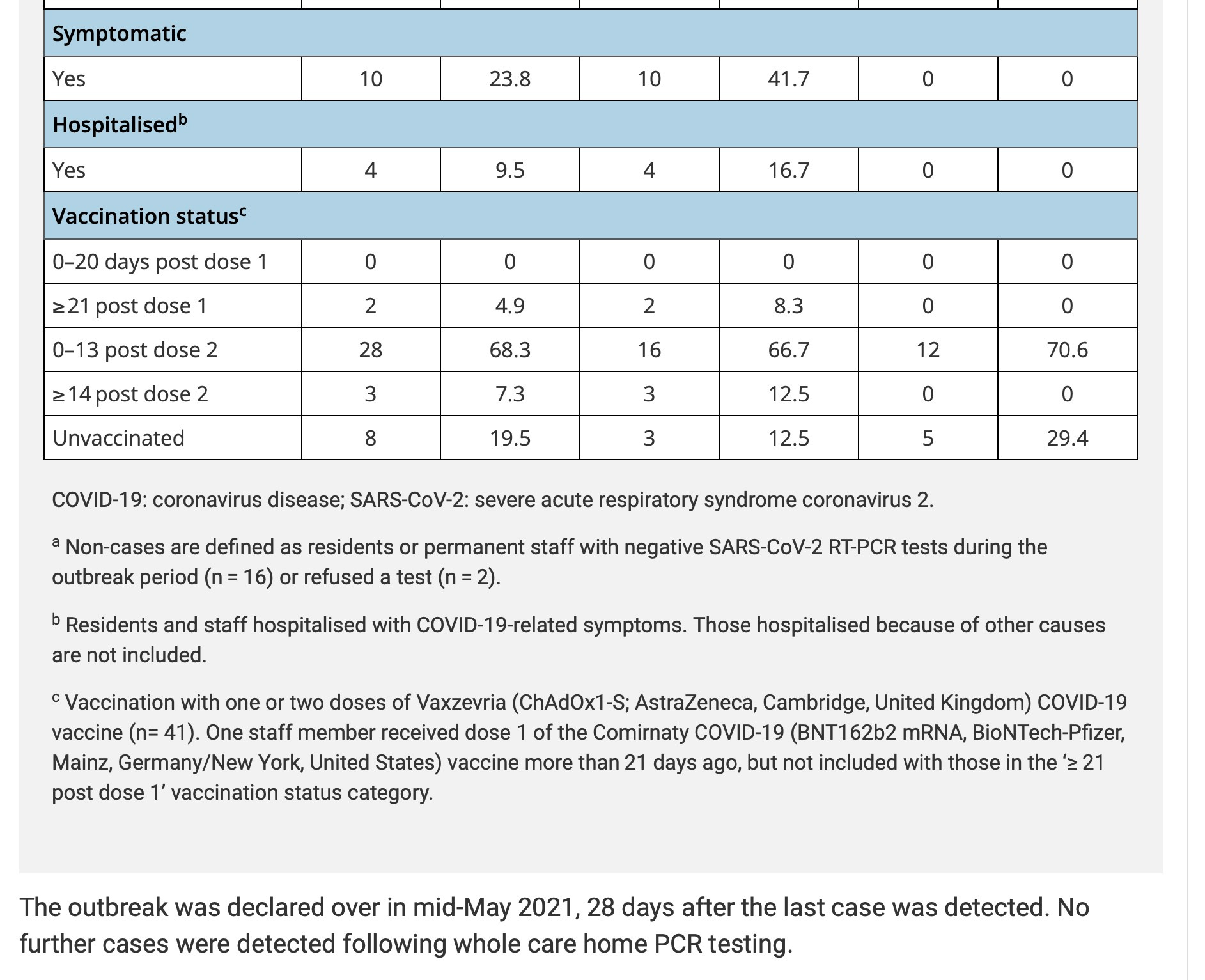
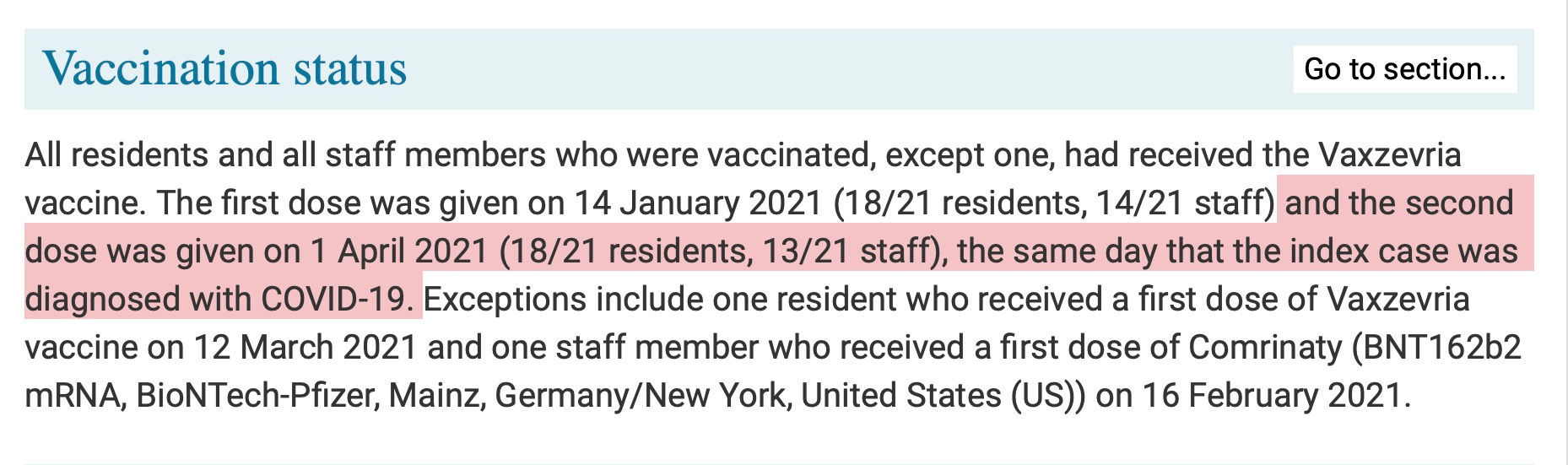
I want to show you that the assumption that the first dose is related to susceptibility is a kind of association fallacy or bias and instead one may susceptible for more complicated reasons than just that, and that a second dose doesn’t make anyone less susceptible than first dose but timing and condition of recipient might matter. In this UK care home study, 87.5% of the infections in the vaccinated happened after second dose but within 14 days, so not counted as vaccinated.
😲
Risk of infection in injected → Infections in Injected (2+16+3) divided by Injections (2+28+3) = 21/33
Risk of infection in injected 3 weeks ago → Infections in Injected 3 weeks ago (0) divided by Injections 3 weeks ago (0) = 0/0
Risk of infection in injected more than 3 weeks ago → Infections in Injected 3 weeks ago (2) divided by Injections more than 3 weeks ago (2) = 2/2
Risk of infection in injected again 2 weeks ago → Infections in Injected again 2 weeks ago (16) divided by Injections 21 days ago (28) = 16/28
Risk of infection in injected again after 2 weeks → Risk of infection in injected again after 2 weeks (3) divided by infection in injected again after 2 weeks (3) = 3/3
Risk of infection in secondary injection exposure → Infections in secondary injection exposed (infected unvaccinated) (3) divided by unvaccinated secondary exposure to injections (8) = 3/8
So VD → Vaccine Danger (Negative Vaccine effectiveness) for Injection vs Non-injection →
Risk of Infection in Injected / Risk of Infection in secondary exposure to Injected
(21/33)/(3/8) = 1.696969696969696969696969…
VE → Vaccine Effectiveness for Fully Vaccinated by world standards vs Unvaccinated
(3/3)/(21/38) = -.8195238095 or -81%
Naturally, we will therefore report that both Fully Vaccinated and Fully Unvaccinated contributed 3 infections each proving beyond doubt that the vaccines are safe and effective since they are at par at 12.5% contribution each to the 100% of the infections.
Conclusion. Get boosted of course. Delta variant infected 57% of the care home and 87.5% of those infections were in the not yet fully vaccinated.
[This was a partially sarcastic computation and tone to show you how the same dataset can be used to spread infections and blame the sufferers of infection and drive viral evolution to places it wouldn’t ever go this easily]
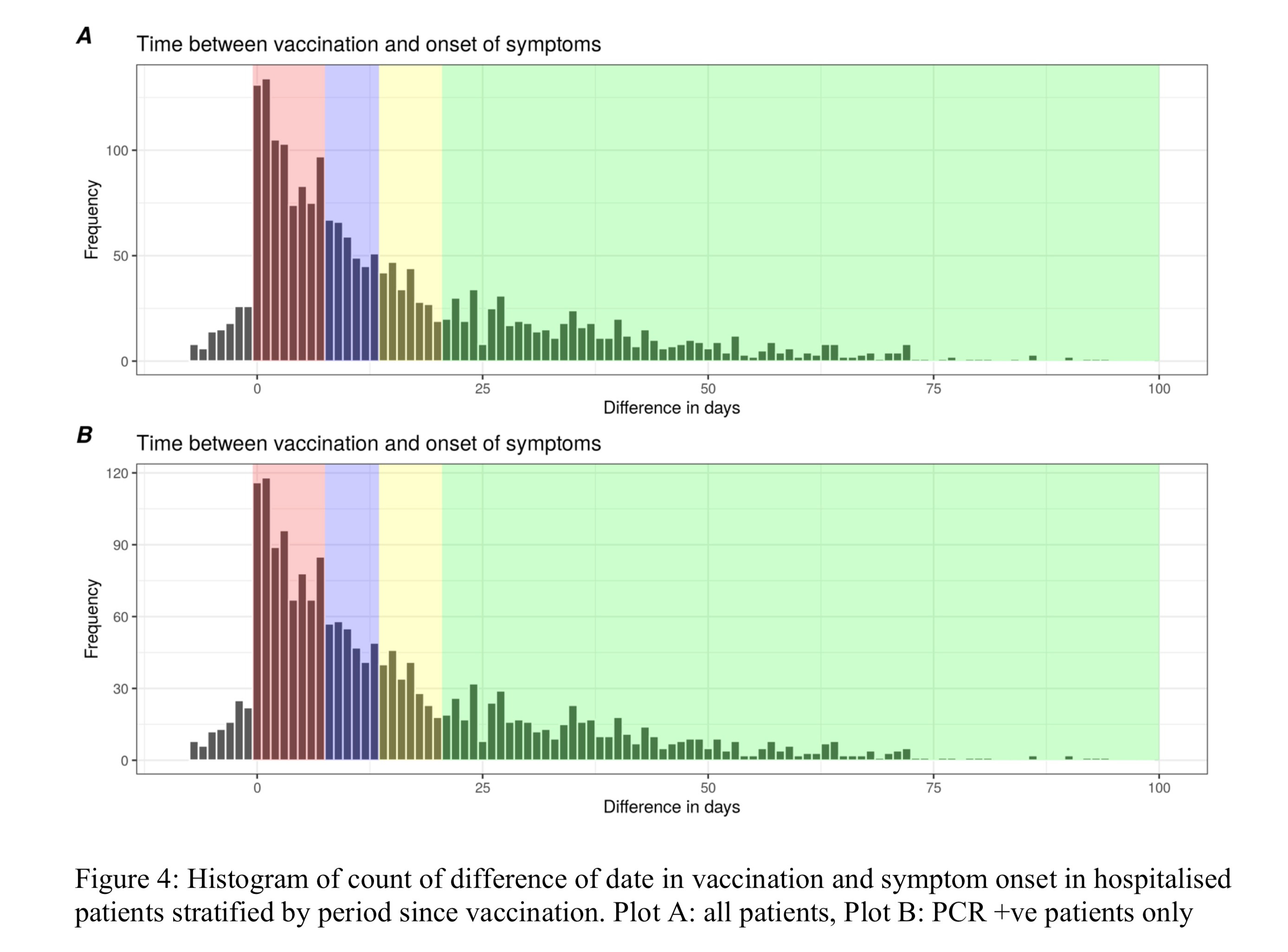
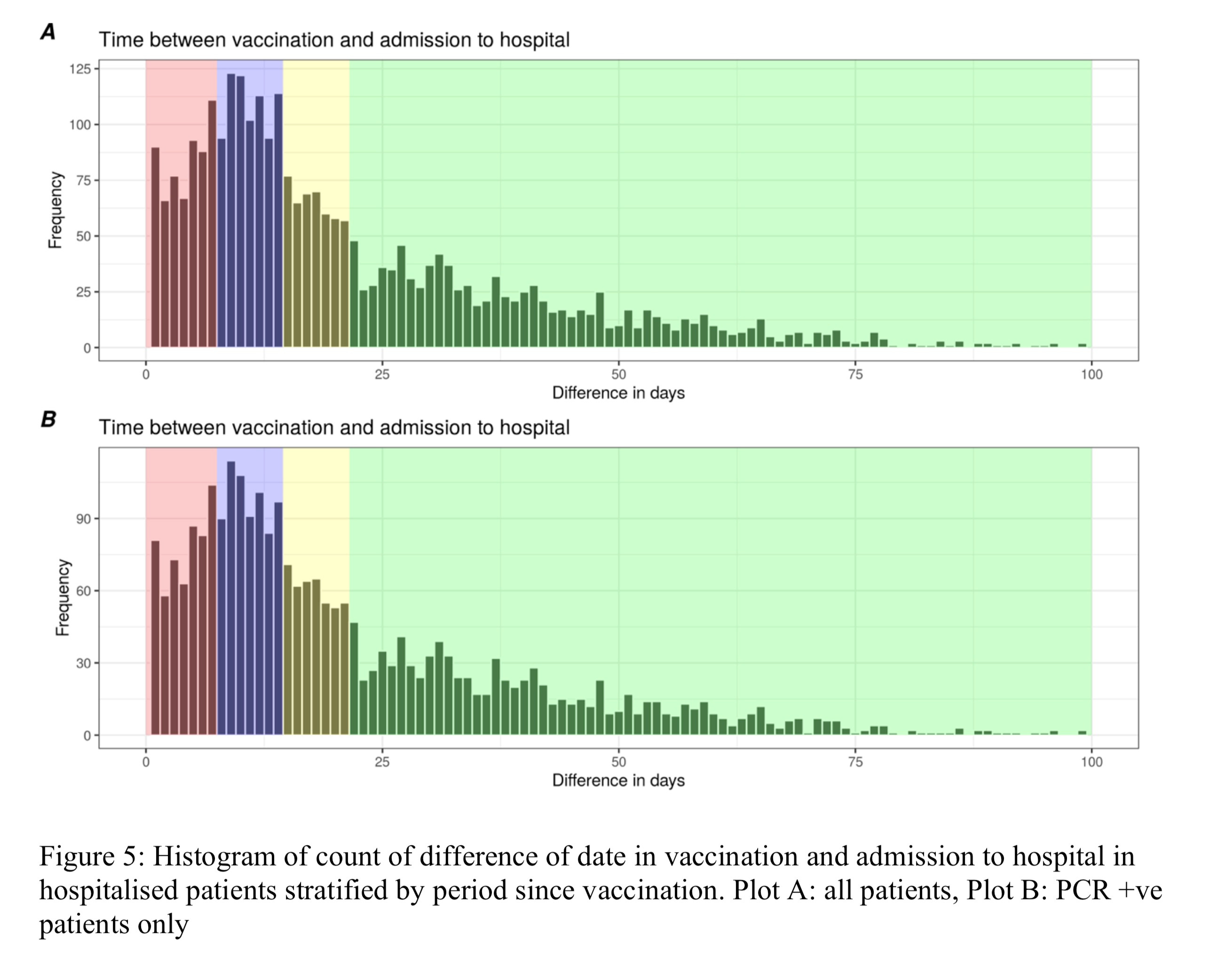
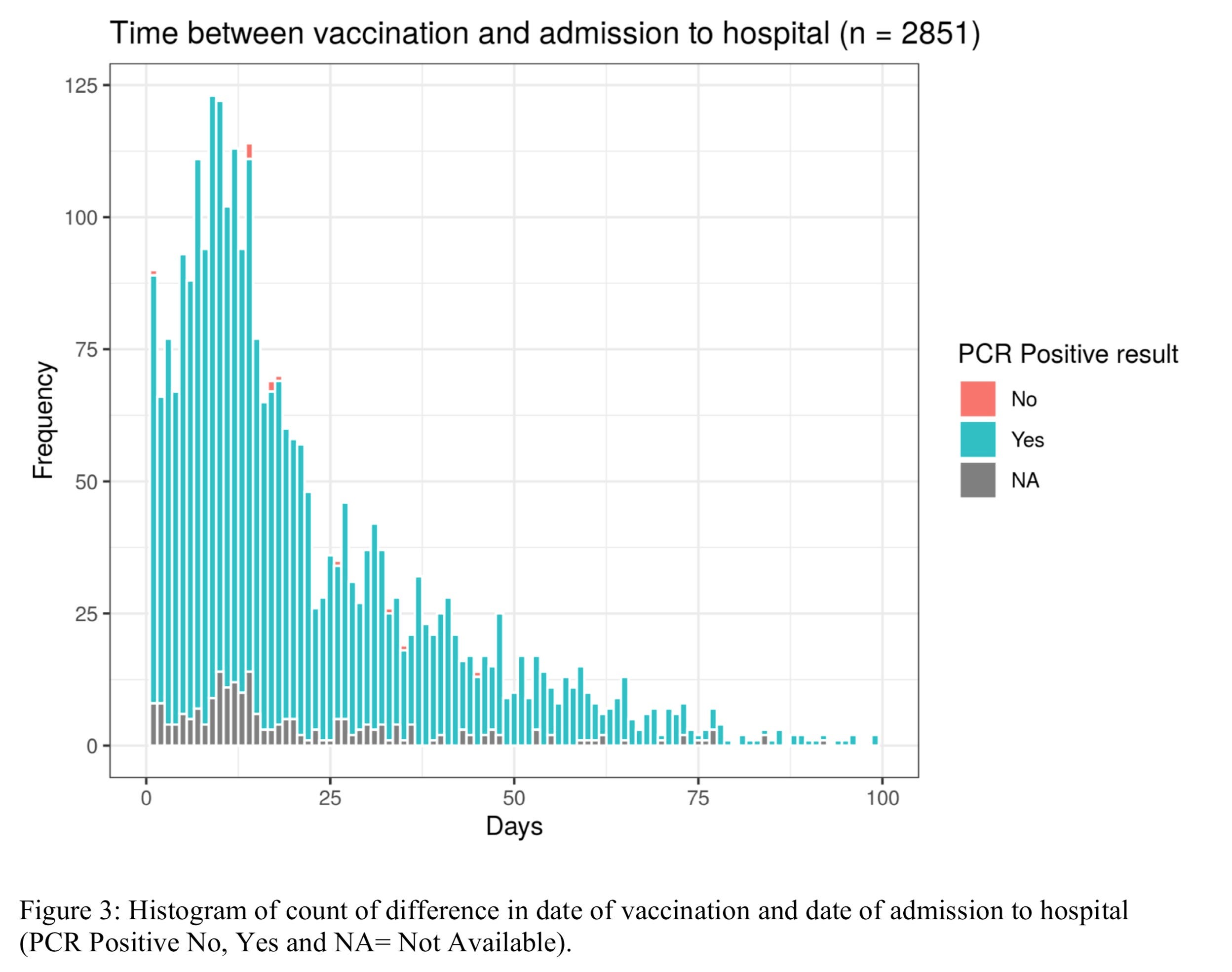
Of course, no need to worry about the 4 hospitalizations, it’s just mild and you know it. And who was hospitalized by vaccination is not needed to be known as you can read the paper and distribution curve to infer it. Same for susceptibility and transmission of variants.
The supplementary index contains all these, of course seropositive unvaccinated are removed from comparison (but not excluded from vaccinated)of secondary attack rate because we don’t want to reach herd immunity and including them would suggest that they could help. Onward transmission is the basis of pandemic(multiplicative) risk vs independent (additive) risks like cancer/car crashes)
Proportions can be misleading if prevalence is rising. Proportions showing vaccine effectiveness.
Prevalence showing vaccine danger. (Killing others not yet treated faster than before you got your treatment but not killing you any less than before, but more.)
Why did something that was appearing to be on it’s way out on December 7th suddenly decide to switch gears?
“It’s the Alpha variant stupid!”
Got it. It decided to show up on December 7th to assist Pfizer’s champagne bottle opening day. What a coincidence. Surely, it’s just hospitals faking the data for “casedemic” right?
Well, if it was a “casedemic” then we would see it in test negative study.
For everyone that tests positive, they find someone who’s in the same “situation” like a doctor or nurse in working in the same covid ward and test them too.)
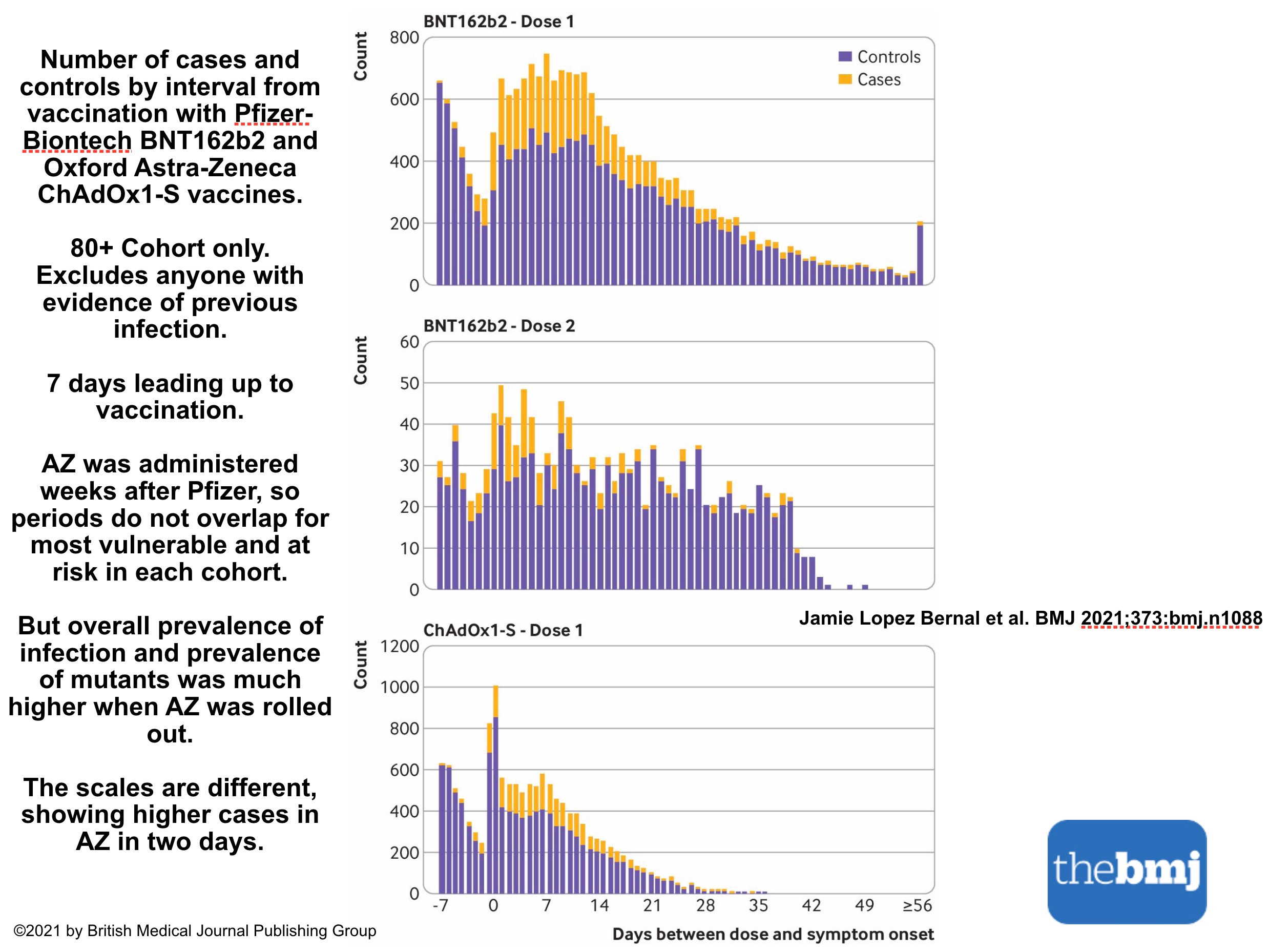
Here’s data for exactly December 1 to 7 prevaccination. Carefully constructed by UK scientists because it’s clear they thought they were seeing the dip and a good chance to sell the enhanced efficacy of the vaccine on the back of a declining curve like Israel tried.
So what happened in England? (Yellow is eventually Injected cohort, Purple is exposed to those before injection and then re-exposed to secondary exposures of shedding from newly injected (Control))
Look at the prevalence (size of epidemic curve) and Susceptibility Enrichment (proportional contribution to wave), look at the shape of the curve (implies causal change due to reversal).
Finally look at the declining curve before the vaccination day. This shows scale invariance. Setting invariance. Even in second dose, the same thing happened the effect size is diminished for all kinds of reasons including not being able to get the same people who died or injured a second vaccine.
Sadly it also was more than just one cohort, it was accumulated each time through fast mass vaccination. Heres proof.
The bump is not an artifact or a coincidence. It has to be causal. If may not be the vaccine, but it sure as hell seems right in the thick of things. If it’s something else and the vaccines are something in the causal pathway, we should consider removing it in the causal pathway to see if it modulates the effect at all.
Thankfully a country tried this. And got good results because their friends from UK didn’t inform them in advance not to administer the second AZ Dose which UK did stop because (well you’ll know in a few weeks). But here’s a preview.
This isn’t a first dose problem as many have tried to simplify it to contain it and minimize it. It’s something far worse, and it might be the method the virus is best at utilizing (thanks to brain dead immunologists and vaccine trial protocol designers and global/local health authority classification incompetence) to learn and disseminate new tricks to gain general fitness.
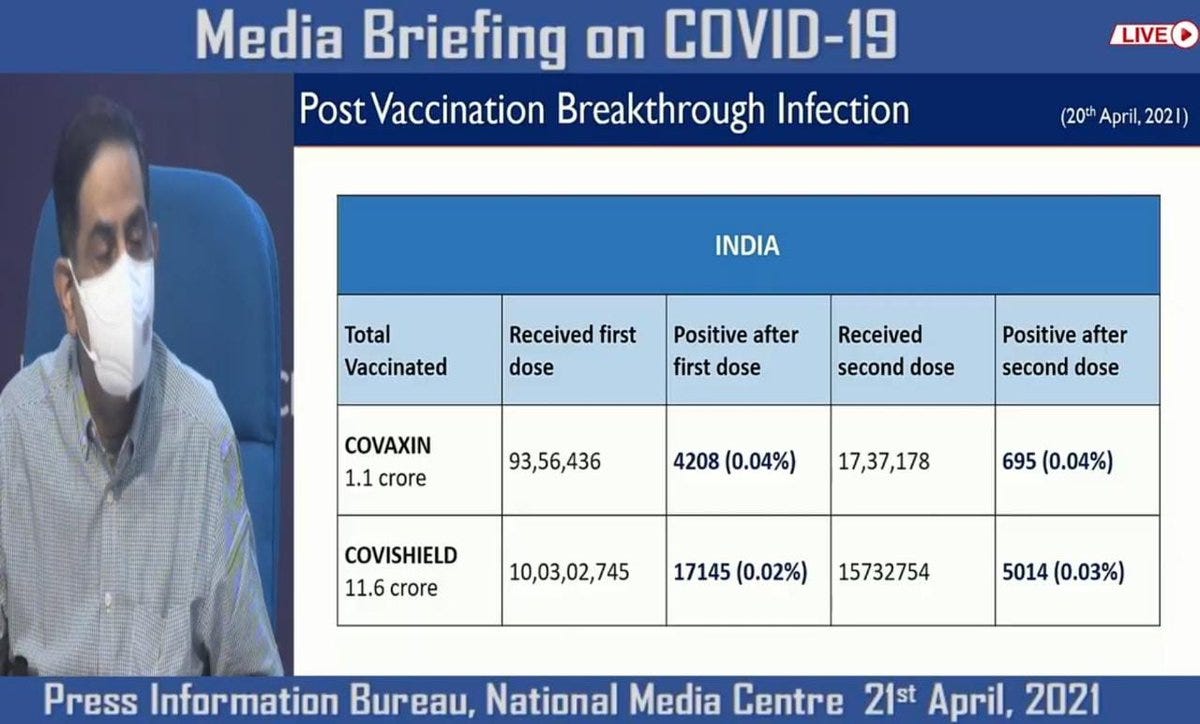
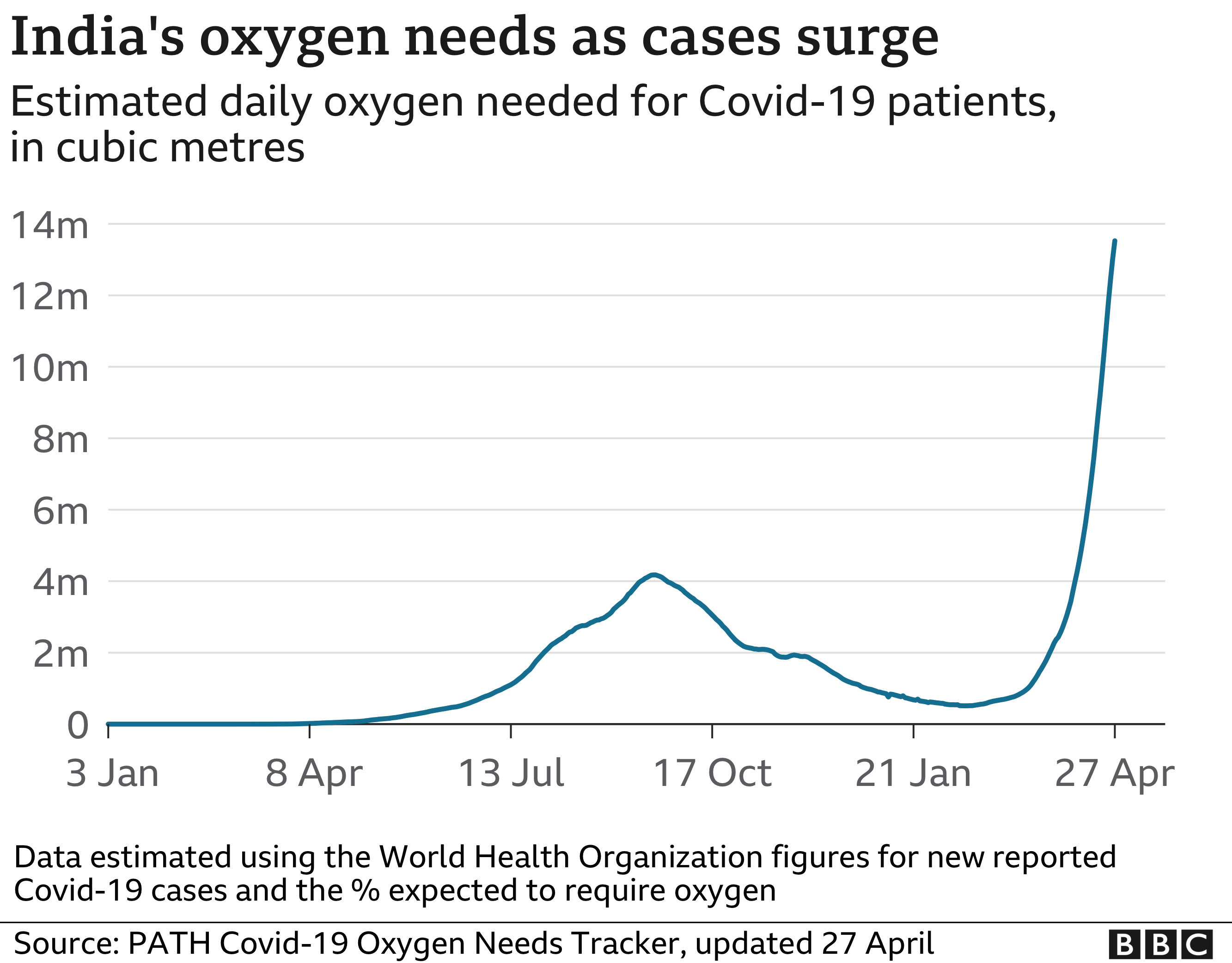
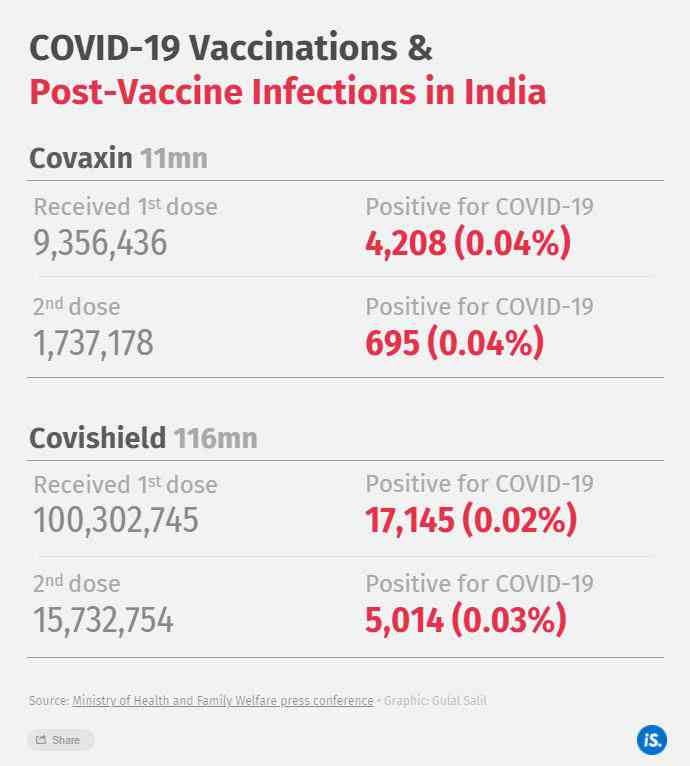
India and Indian Medical Authorities were under the impression that 2 is better than 1. They proved this using this graphic that Indian print and digital media shared with the world showing them the vaccines were working.
Notice, the numeric separators are removed for 2nd doses of AZ (Covishield). This is a well known trick along with “Absolute risk” and decimal rounding to try to obfuscate data in front of your eyes.
Since the absolute risk is tiny, why should I care if .02% looks smaller than 0.03%. that’s a 99.97 survival rate!
Curious that this being touted as a success. Of course, because we implicitly think a small number cannot become big and even if it can, it’s as just noise. How could the first dose have better efficacy that then second?
Well 5000 cases is not random chance. And in my view, that’s
Vaccine Danger = 186% increase in cases if you repeat this several million times.
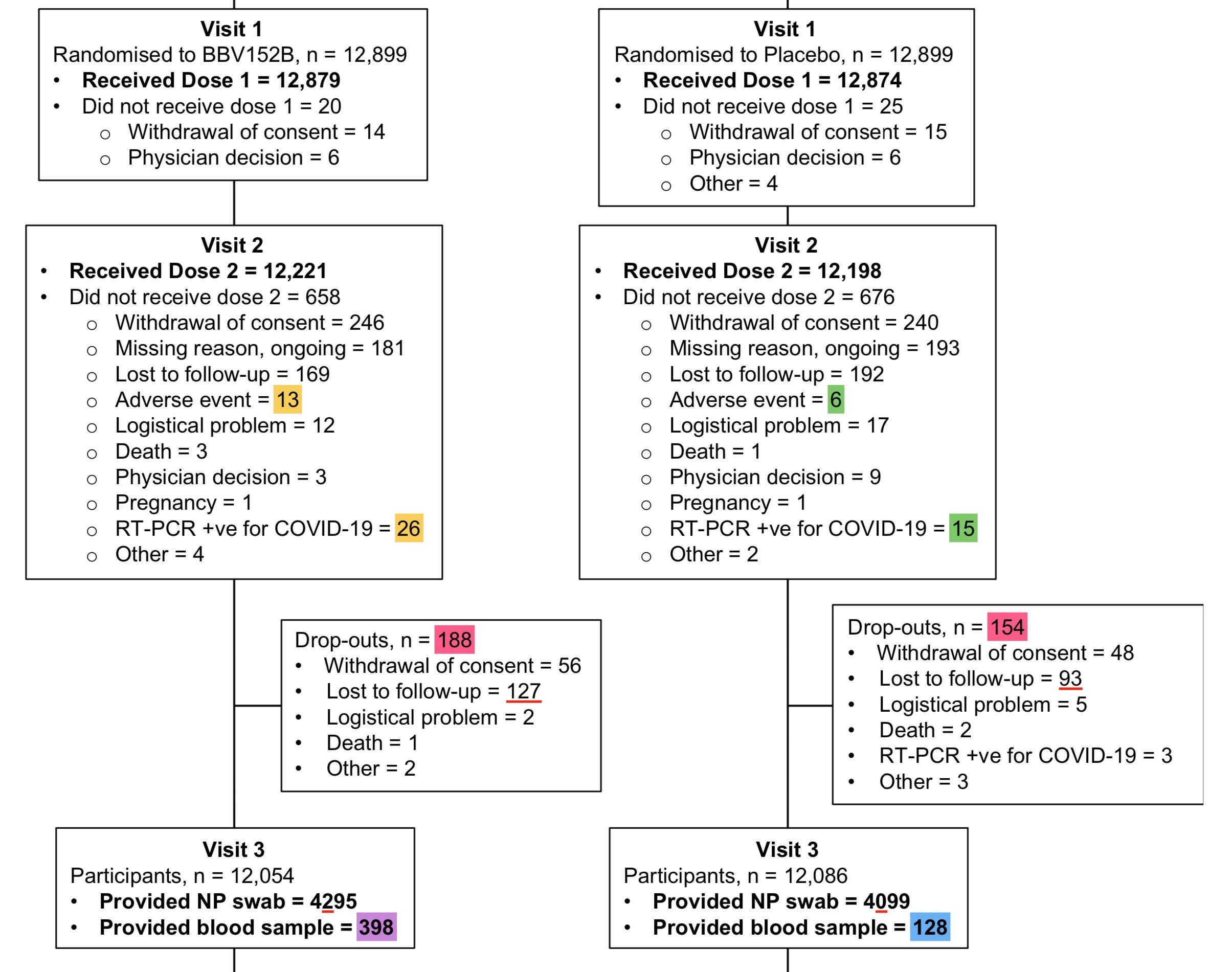
COVAXIN the other vaccine being administered looks better only because it achieved Vaccine Danger in it’s first round itself. Look at the trial data showing 73% more cases in treatment arm.
Still. It’s weird that even then Covaxin had a negative effectiveness and vaccine danger of 112% compared to 173% in dose 1 from the trials. [1-(4208/9356436)/(695/1737178)=-.12] which is about what Pfizer’s trial shows the vaccine danger is for baseline PCR positive.
“Absolute Risk” fans may not like what I just said but one has to understand that absolute risks are not always additive, if they are multiplicative and the order of events matters, we’ll see an effect size unlike anything ever witness.
Check→ What happens when vaccines of different types and different levels of infection promotion capabilities are introduced massively from most vulnerable first to younger fitter age groups.
But we should boost only when we understand precisely what these types of vaccines do, when they do it, when they interact with each other in a population and during rapid deployment.
Soon we will have billions of doses ready. And unlike last time in India where they ran out of vaccines and that accidentally stopped the mass vaccination campaigns. We may not have the time this time around. We have to equip ourselves to see through the hypnosis and data obfuscation.
The trials openly show negative efficacy and nobody cares.
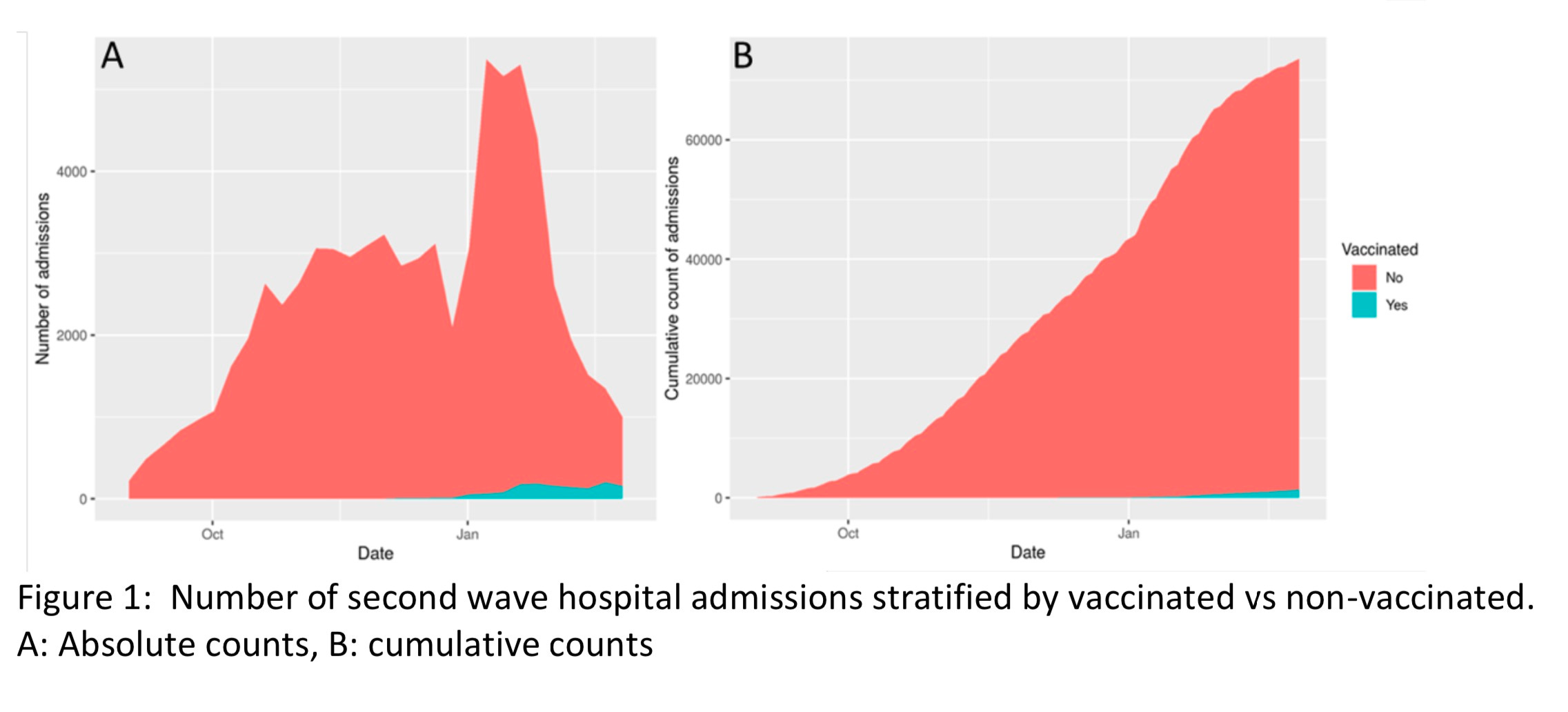
Let’s go back to that England Hospitalization data from last year:
This will could happen to younger and younger people what you see in this graph if we don’t get a clearer idea of why this virus quickly capitalises on multitude of settings, low or background infection, higher lower temperature, seasonal peaks, reservoirs, induced antibodies, vaccinal or otherwise to gain access to improve fitness very rapidly. Maybe all of it is vaccines, maybe it’s co-incidental. But we are just ignoring our children’s future without knowing if we are carving a giant that we won’t be able to kill.
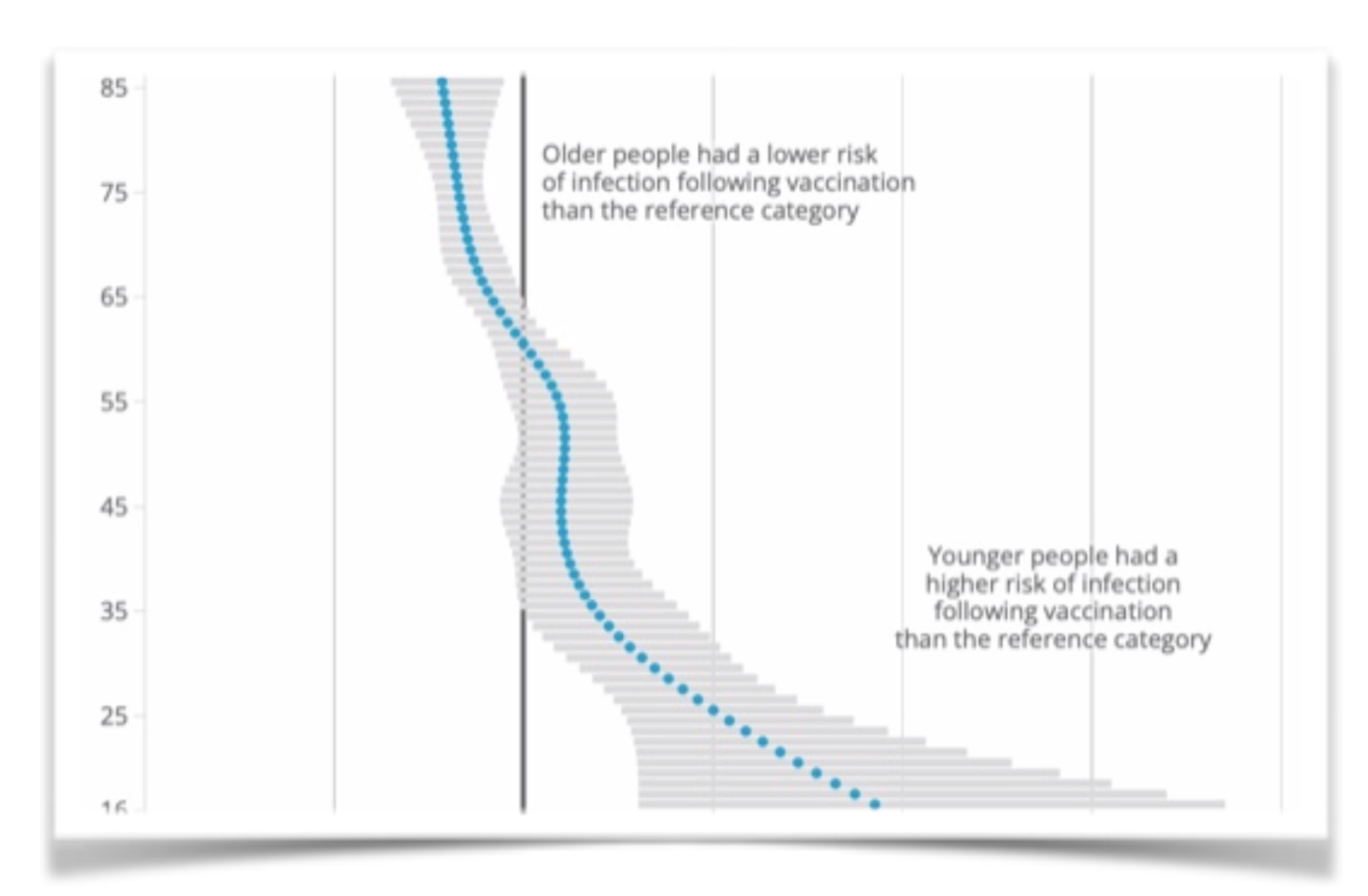
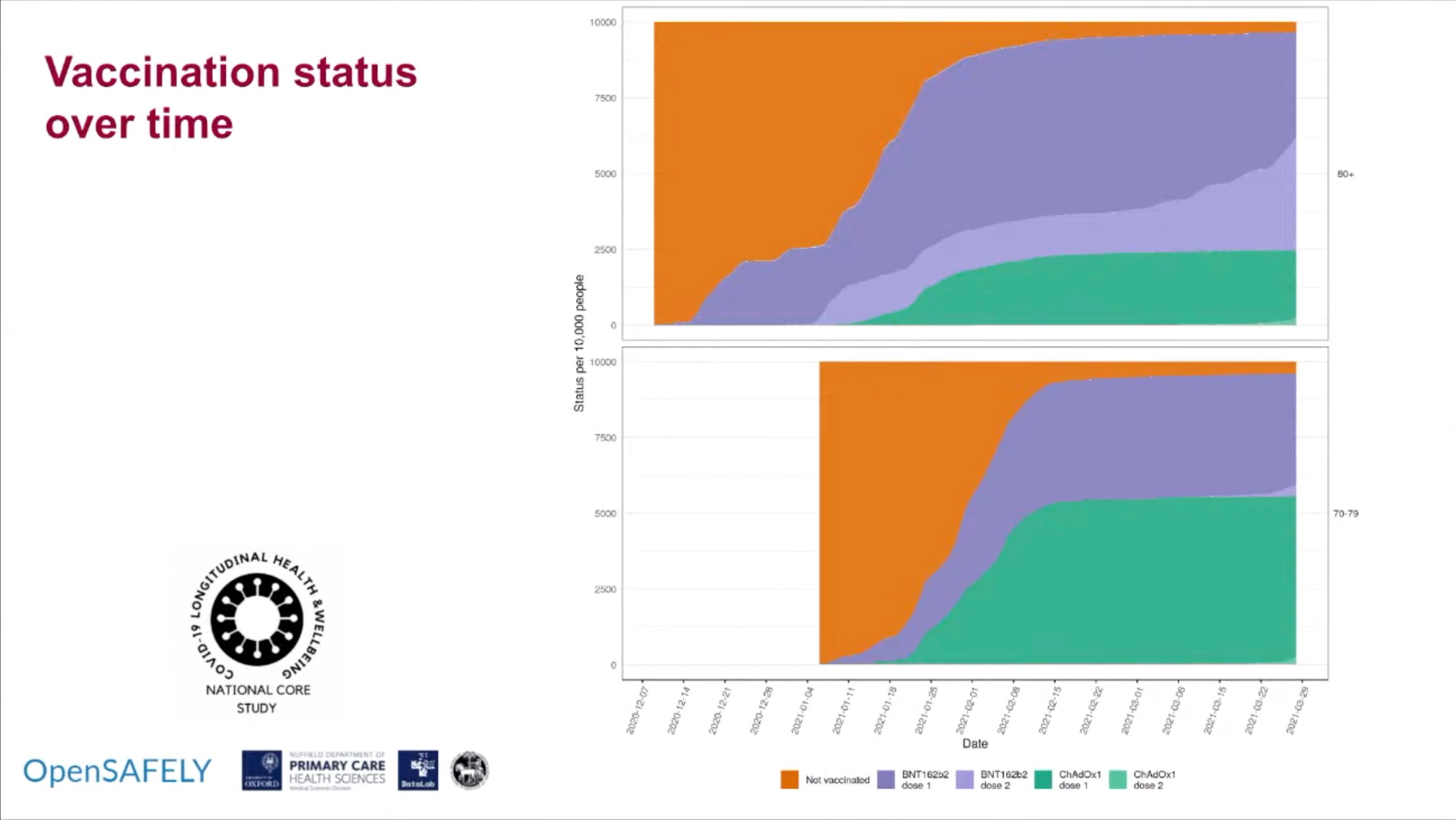
Over 80’s vaccine. The control group has been eliminated. Now we have to hope that many of our triple vaccinated peers will want to investigate the evolution of this pademic with the same kind of seriousness the others wanted. They will now be the victims of statistical gaming and labelling errors and rapid elimination of controls.
Why does that negative efficacy (Vaccine danger) number for delta hover around -80%?
Is that a one time phenomenon or something fundamental the virus does each time under pressure?
Here once again the virus used the first dose to generate variation by enhanced susceptibility, and the second dose was used by the virus to select a fitter form that it could easily magnify in other vaccinees. Perhaps vaccinees that saw a slightly altered spike protein like AZ.
If it can do it each time, then what can we do detect that it is doing it and reverse course? If this is just some mathematical effect of biological systems then we are screwed unless we luck out or the primary driving force behind this suddenly reaches a global maxima without revealing why or how. The best we can do is try to break it apart with raw data and not aggregate picture of things where things can appear great “on average”.
All while this amazing pattern is repeated over and over where strong selection pressure is applied by those with antigenic experience, the vaccination creates conditions for it to quickly multiply unchecked either through vulnerable being differentially attracted to vaccines in this phase or the vaccine itself depleting the immunity as has been shown in multiple studies.
Enhanced susceptibility, Massive replication and shedding of new mutations, onward transmission by others. Then strong selection pressure and differential uptake of the fittest. Every dose in every human might be doing this independently and forming a massive cascade…
—
If we don’t demand better data and non-aggregation of events and minuscule specificity and non censoring of events, the virus will find a way before we can find the way to know how it persists.
Right now it’s obvious, the virus has one trick that it’s used for the last year to grow in presence - the extremely naive “Vaccination” category that includes the benefits of being termed unvaccinated when caught while being “vaccinated” when not. This will obviously do things like this to adjust incubation time and shedding dynamics. The virus responds to our infection control + unobserved time.
Either we stop our infection control measures or if we are continuing them then we must dutifully observe without wasting a single second or hour trying to “prove” things to the public or if the data will look good or bad. Not everything has to be about who was right or wrong and short term elections and promotions and salaries. Sometimes, we just have to do what’s logical for our long term benefit. Right now, obfuscation is highly detrimental because we are blinded being led into a place we won’t be able to return back from.
The virus has to work within the constraints we put on it. Not observing it at all is a better constraint than forcing it in places where it can’t be observed. We will just create problems we cannot fix if we continue at this rate. It’s not an accident that delta variant had a 13.2 days generation time while other variants 4. It’s because its trying to evade the stupid "14 days until you are fully protected!" rule.
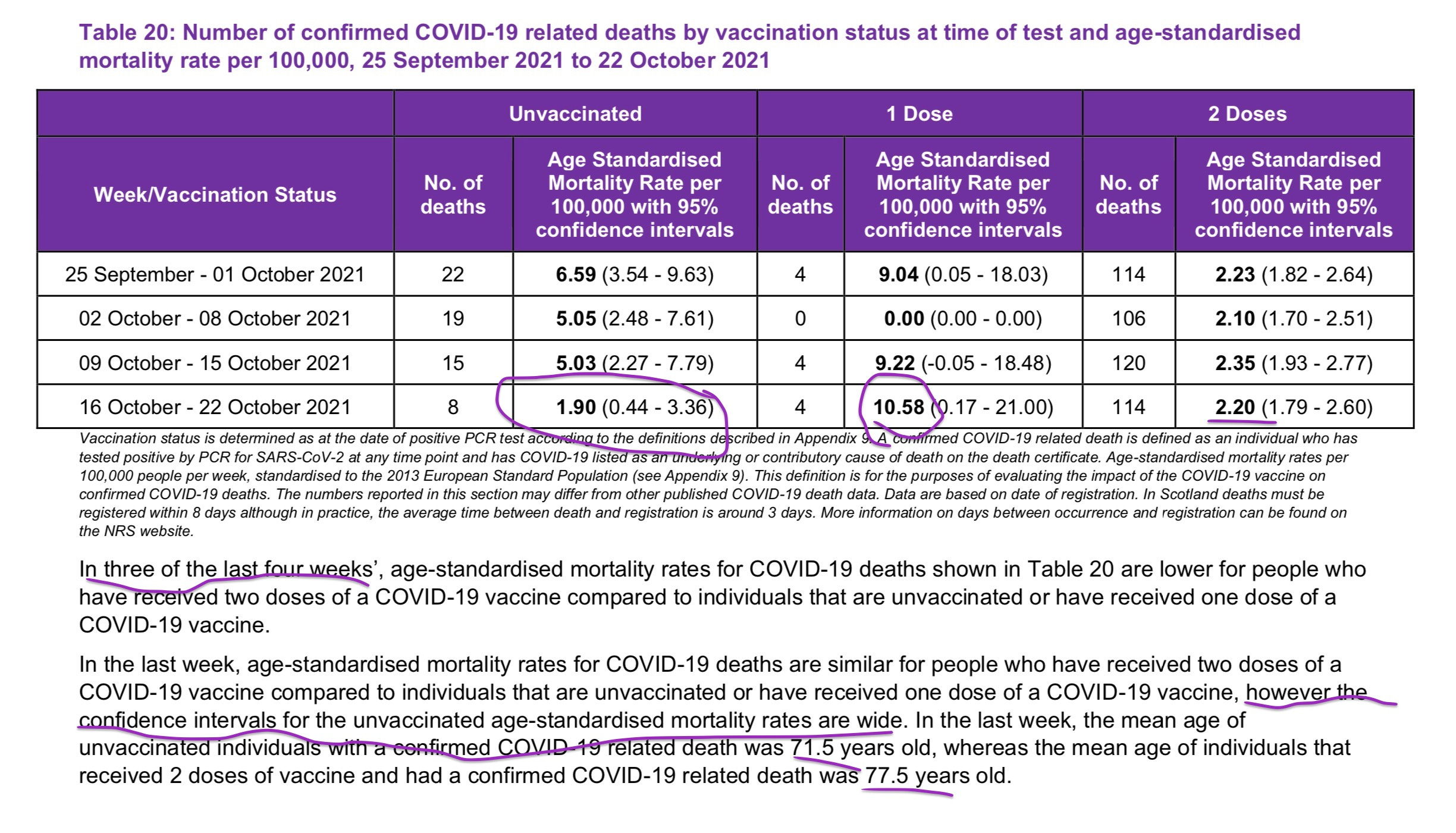
So the virus is killing younger people on average this year and even younger in the partially vaccinated and we are cool with that because they are classified as unvaccinated and nobody cares. So the entire theory that the vaccine is going to add years of lives lost back has not happened in Scotland or anywhere else. So the solution is to boost and vaccinated children.
Got it.
If we keep trying to game the system to hide the truth, the viruses that can game the new rules probably already exist anyway, just waiting in the wings to take over when we make that mistake. Don’t elongate incubation time, don’t select for viruses that shed fecally by focusing completely on nasal swabs. We will force the virus to exist and infect things we don’t want it to.
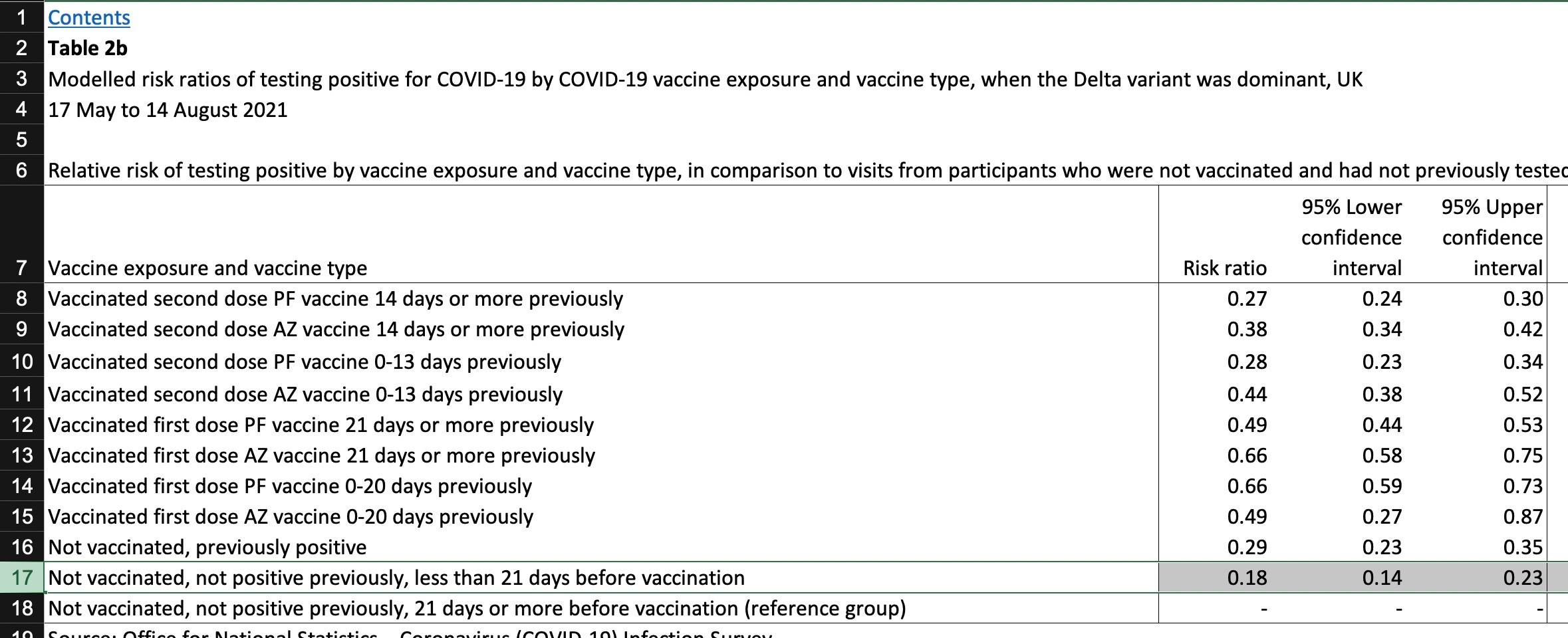
It should be mentioned to everyone that the safest and healthiest moment in their life was the 21 days before the vaccination according to UK infections report.
Not a single soul inside the agency has the pressure to explain the interesting choice of “reference” group.
“Not vaccinated, not positive previously, less than 21 days before vaccination”.
This is the definition of “Dynamic Rigging’. The rigged stats, the rigged labelling, the rigged classification, the rigged “regression models” without acknowledging causal pathway between injection to new infections making the calculation look more absurd every time.
This is going to end with the virus elongating it’s incubating period or shedding because the pressure is being put that way due to dumb modelers and corrupt medical establishment not acknowledging the real source of infection persistence and promotion. Our own dumb policies and massive interventions and addiction to misrepresentation and outright lies using sophisticated detection protocols that were engineered through trial and error in early 2020, with the support of a completely corrupted media establishment and steady source of people in psychological and physical vulnerability who will do anything to feel good.
The incubation time is not a constant, the disease transmission and attack rates are not constants, the “r” is not a constant, the symptom onset is not a constant, the symptom set is not a constant, the damn virus is not a constant. You cannot outrun it with these completely unhinged policies. The virus can outrun though.
Keep Boosting.
Let’s try to unmagnify fear and paranoia through asking for simple things from people who are willing to help. I think Meaghan Kall from UKHSA does a great job interfacing with the publc and she might be able to help with the data we need to identify risks and eliminate them.
Hopefully others will see what we can see before the virus becomes unstoppable through acquiring fitness it would gain in 900 billion infections over 1000 years within a span of a few months if we start boosting children 0-4 with non-sterilizing vaccines which is inevitable given China has already done it to 3 year olds and India has announced 2-18 year olds.
More on reinfections written before asking for stratification by seropositivity:
"Hopefully others will see what we can see before the virus becomes unstoppable through acquiring fitness it would gain in 900 billion infections over 1000 years within a span of a few months if we start boosting children 0-4 with non-sterilizing vaccines which is inevitable given China has already done it to 3 year olds and India has announced 2-18 year olds."
Thanks, I will reply to your other posts in a bit. Fixing the post first, as I want us to have this data included before it starts to look worse and worse for the vaccine if it does go in that direction.
"You may have heard from many who noticed that susceptibility is higher after the first dose of vaccination for a few weeks.
I want to show you that the assumption that the first dose is related to susceptibility is a kind of association fallacy or bias and instead one may susceptible for more complicated reasons than just that, and that a second dose doesn’t make anyone less susceptible than first dose but timing and condition of recipient might matter. In this UK care home study, 87.5% of the infections in the vaccinated happened after second dose but within 14 days, so not counted as vaccinated."
Let me check double-check that I understand the claim (hypothesis) that you are making. As I understand it, your premise is that people are more susceptible to infection after the virus immediately after each dose (than they were immediately before the dose). Correct so far? That is actually an easy hypothesis to validate with causal significance if we only had a modicum of granular-enough data... which we do not have. The people that have the data seem unwilling or incapable of doing that.. or maybe both. Unclear.
I have long suspected this is the case, personally (from a logical perspective), and your look at the data seems to back this up. But you are also, again if I am not mistaken, saying that the (let's call it) change in susceptibility after the second dose may equal the change after the first dose. That is an extremely hard thing to quantify for a variety of factors, but I will push back on it nonetheless. We can clearly see the first dose leads to negative VE in many different cases across countries and seemingly regardless of situation (except if the virus either does not exist in the population being measured). We do not see the same in the second dose. In fact, we see relatively high VE in many cases. Some of that may be for the reasons you mentioned... but there is another reason that all but guarantees susceptibility is lower after the second dose: the second dose follows the first.
In other words, the first dose makes populations susceptible to the virus, and thus, we are eliminating many candidates from the pool of possible infections during that time period. Infection may not be as robust in the vaccinated as those with natural immunity, but it is still relatively robust. So the second dosers are necessarily less susceptible. Now, if we are talking about a virus naive population, or a single individual, or a small study, this may be true. We can probably even see this in populations like Singapore that had few infections until the population was heavily vaccinated. I wonder if there is data available from there? But I would still be reluctant to believe that the second dose would be equal to the first in this regard (assuming their immune systems learned something from the first dose and susceptibility will be somewhat offset by that learning).
I don't know -- maybe I am missing the point or making a bad point. Or maybe the truth is staring me in the eye and it is too horrific to believe as it would imply we will be living this never ending story as long as they continue to give boosters. Feel free to correct my errors in logic as I am not sure I fully grasp the meaning here.
Wow. that took 3 hours or more but I updated with the granular data. Do you think it makes the case that this the first event and last event in any case study cannot be assumed to be equally likely?
The virus's best friend will always be the infection promotion measures we instate using elected representatives with our tax money helping to spread the virus via vaccine.
This amazing plan of NOT TESTING ONLY WHEN BOOSTED is literally what the virus would have requested people to do if it wanted to become unstoppable. How can we show objectively that more vaccine has not proven to lead to less virus yet. Is there any limit at which we will think "More vaccine is leading to more virus, even though it's 99% efficacious, that can't possibly be right. Let's stop and think about this."
To clarify, I am not saying the first and second doses are equally likely to produce the same outcome, but that any dose is capable of producing the outcome we associate with a specific dose.
For example: We could associate 1 dose with high infection risk for a short time and then drastically lower fears of infection after, especially not after the second dose permanently. This could appear immunologically and empirically true but could be a sampling artifact of the conditions that existed when the first doses were administered globally and the how that changed the landscape rapidly. The second dose may have done the same thing if the population level dynamics were reset to the same state. In this specific case- Astrazeneca second dose was not given and 12 week gap was added because I suspect they realized quickly that Pfizer and AZ are having some kind of negative interaction at the population level. That is not an accident because the thrombosis risk was cited for the pause of 12 week but in reality I believe they saw what India would find out a few months later. The second dose infected more prolifically than the first. There is a suspicion that this could be because AZ killed the susceptibles before they could be infected and only the strong survived for the second but this doesn't explain why this was also the case for the other vaccine whole virus vaccine co-administered (Covaxin) which also had negative efficacy compared to first dose. The easier answer is that the first dose in India was administered during a time of low prevalence and off season without a specific push to find and vaccinate vulnerable. They may have been more susceptible to infection, but there wasn't much virus around to infect them. This changed dramatically when slowly Delta acquired the mutations it needed by serial passaging in newly vaccinated double dosed in late march. Then India kicked into season due to heat -> air-conditioning. BooM. So this way, the first dose couldn't do anything that bad to you other than personal side-effects but it allowed something worse than that, it allowed for people to think they were protected and that allowed delta to be quickly selected and massively spread upon the second dose which would of course only attract the most vulnerable and likely already exposed first. Then cascade begins of people not knowing that the virus engineered a way to attract only those it can infect exactly where and when it can infect them and no-one else. The vaccine didn't change. Only the conditions and virus changed to adapt to whatever best suits persistence and spread. In india, that was subliminal spread with 1 dose and terrorizing spread with second. Noteworthy that one small island territory off the coast of india had zero cases all pandemic and on January 16th they administered the first vaccine and January 18th they had the first cases. That lead to 10,000 cases but most after the second in the delta wave. So the vaccine appears to do exactly the same thing each time, we just change our setting and timing and sometimes it goes horribly wrong, and when it does, the vaccine gets the most uptake and so does the virus. Total amount of virus copies and vaccine injected today is exponentially higher than when this started, and the rate is just increasing.
I still have twitter, just to be clear, you want me to reply to Igor's comment and write:
“reinfection not just by vaccination status but days since last injection status so that reinfection impact due to immunization is seen clearly possible to judge especially susceptibility in the first 3 weeks.”
Is that right? Sorry for being dense, just want to ensure I am doing this correctly.
And No no, you are not dense, I'm a better writer than a thinker, and I am absolutely terrible at writing and loathe the concept of proof-reading my own words as it causes me to over-correct and tunnel into random branches like Trump at his rallies.
I think just letting the requester know that you also think this would be useful for everyone to follow around the world, if you feel so, then it might spur the agency to include it. Everyone wants to feel helpful and demanded. UKHSA is no different. So just write whatever you wish, or nothing at all but be authentic as it's not right to overrepresent a minority of one (me).
Thanks so much for asking. I'll fix my post, but I don't need you to write back to anyone at all. Just supporting his request with a "like" is sufficient. I think I will remove the request for more info. If Meghan (the person who is likely going to push the agency to include stratification by public interest shown) gets a sense that something or someone is coordinating this request then she might become skeptical of its utility. I don't want to push people who are willing to give the public information, if they can as long as they don't realize in advance that those same data classifications could be detrimental to the public health campaigns current advocated strategy in the future if the numbers show something they didn't expect. This is why we need to get them to include those numbers now before the "trend line" becomes clearer. As you know, when the trend line shows something they didn't expect, they will censor it. So best is to act early for transparency, without malice or agenda. Just data.













"Hopefully others will see what we can see before the virus becomes unstoppable through acquiring fitness it would gain in 900 billion infections over 1000 years within a span of a few months if we start boosting children 0-4 with non-sterilizing vaccines which is inevitable given China has already done it to 3 year olds and India has announced 2-18 year olds."
Horrifying on every level.
Thanks, I will reply to your other posts in a bit. Fixing the post first, as I want us to have this data included before it starts to look worse and worse for the vaccine if it does go in that direction.
I have a feeling I know what you are talking about, thank you.
Post updated.
"You may have heard from many who noticed that susceptibility is higher after the first dose of vaccination for a few weeks.
I want to show you that the assumption that the first dose is related to susceptibility is a kind of association fallacy or bias and instead one may susceptible for more complicated reasons than just that, and that a second dose doesn’t make anyone less susceptible than first dose but timing and condition of recipient might matter. In this UK care home study, 87.5% of the infections in the vaccinated happened after second dose but within 14 days, so not counted as vaccinated."
Let me check double-check that I understand the claim (hypothesis) that you are making. As I understand it, your premise is that people are more susceptible to infection after the virus immediately after each dose (than they were immediately before the dose). Correct so far? That is actually an easy hypothesis to validate with causal significance if we only had a modicum of granular-enough data... which we do not have. The people that have the data seem unwilling or incapable of doing that.. or maybe both. Unclear.
I have long suspected this is the case, personally (from a logical perspective), and your look at the data seems to back this up. But you are also, again if I am not mistaken, saying that the (let's call it) change in susceptibility after the second dose may equal the change after the first dose. That is an extremely hard thing to quantify for a variety of factors, but I will push back on it nonetheless. We can clearly see the first dose leads to negative VE in many different cases across countries and seemingly regardless of situation (except if the virus either does not exist in the population being measured). We do not see the same in the second dose. In fact, we see relatively high VE in many cases. Some of that may be for the reasons you mentioned... but there is another reason that all but guarantees susceptibility is lower after the second dose: the second dose follows the first.
In other words, the first dose makes populations susceptible to the virus, and thus, we are eliminating many candidates from the pool of possible infections during that time period. Infection may not be as robust in the vaccinated as those with natural immunity, but it is still relatively robust. So the second dosers are necessarily less susceptible. Now, if we are talking about a virus naive population, or a single individual, or a small study, this may be true. We can probably even see this in populations like Singapore that had few infections until the population was heavily vaccinated. I wonder if there is data available from there? But I would still be reluctant to believe that the second dose would be equal to the first in this regard (assuming their immune systems learned something from the first dose and susceptibility will be somewhat offset by that learning).
I don't know -- maybe I am missing the point or making a bad point. Or maybe the truth is staring me in the eye and it is too horrific to believe as it would imply we will be living this never ending story as long as they continue to give boosters. Feel free to correct my errors in logic as I am not sure I fully grasp the meaning here.
Excuse all of my grammar errors in the above post. Substack needs an edit button for the comment section.
You are going to love this update to the post in the next 3 minutes. Basically yes!
Wow. that took 3 hours or more but I updated with the granular data. Do you think it makes the case that this the first event and last event in any case study cannot be assumed to be equally likely?
The virus's best friend will always be the infection promotion measures we instate using elected representatives with our tax money helping to spread the virus via vaccine.
This amazing plan of NOT TESTING ONLY WHEN BOOSTED is literally what the virus would have requested people to do if it wanted to become unstoppable. How can we show objectively that more vaccine has not proven to lead to less virus yet. Is there any limit at which we will think "More vaccine is leading to more virus, even though it's 99% efficacious, that can't possibly be right. Let's stop and think about this."
https://twitter.com/disclosetv/status/1470755078449639429?s=20
To clarify, I am not saying the first and second doses are equally likely to produce the same outcome, but that any dose is capable of producing the outcome we associate with a specific dose.
For example: We could associate 1 dose with high infection risk for a short time and then drastically lower fears of infection after, especially not after the second dose permanently. This could appear immunologically and empirically true but could be a sampling artifact of the conditions that existed when the first doses were administered globally and the how that changed the landscape rapidly. The second dose may have done the same thing if the population level dynamics were reset to the same state. In this specific case- Astrazeneca second dose was not given and 12 week gap was added because I suspect they realized quickly that Pfizer and AZ are having some kind of negative interaction at the population level. That is not an accident because the thrombosis risk was cited for the pause of 12 week but in reality I believe they saw what India would find out a few months later. The second dose infected more prolifically than the first. There is a suspicion that this could be because AZ killed the susceptibles before they could be infected and only the strong survived for the second but this doesn't explain why this was also the case for the other vaccine whole virus vaccine co-administered (Covaxin) which also had negative efficacy compared to first dose. The easier answer is that the first dose in India was administered during a time of low prevalence and off season without a specific push to find and vaccinate vulnerable. They may have been more susceptible to infection, but there wasn't much virus around to infect them. This changed dramatically when slowly Delta acquired the mutations it needed by serial passaging in newly vaccinated double dosed in late march. Then India kicked into season due to heat -> air-conditioning. BooM. So this way, the first dose couldn't do anything that bad to you other than personal side-effects but it allowed something worse than that, it allowed for people to think they were protected and that allowed delta to be quickly selected and massively spread upon the second dose which would of course only attract the most vulnerable and likely already exposed first. Then cascade begins of people not knowing that the virus engineered a way to attract only those it can infect exactly where and when it can infect them and no-one else. The vaccine didn't change. Only the conditions and virus changed to adapt to whatever best suits persistence and spread. In india, that was subliminal spread with 1 dose and terrorizing spread with second. Noteworthy that one small island territory off the coast of india had zero cases all pandemic and on January 16th they administered the first vaccine and January 18th they had the first cases. That lead to 10,000 cases but most after the second in the delta wave. So the vaccine appears to do exactly the same thing each time, we just change our setting and timing and sometimes it goes horribly wrong, and when it does, the vaccine gets the most uptake and so does the virus. Total amount of virus copies and vaccine injected today is exponentially higher than when this started, and the rate is just increasing.
I still have twitter, just to be clear, you want me to reply to Igor's comment and write:
“reinfection not just by vaccination status but days since last injection status so that reinfection impact due to immunization is seen clearly possible to judge especially susceptibility in the first 3 weeks.”
Is that right? Sorry for being dense, just want to ensure I am doing this correctly.
And No no, you are not dense, I'm a better writer than a thinker, and I am absolutely terrible at writing and loathe the concept of proof-reading my own words as it causes me to over-correct and tunnel into random branches like Trump at his rallies.
I think just letting the requester know that you also think this would be useful for everyone to follow around the world, if you feel so, then it might spur the agency to include it. Everyone wants to feel helpful and demanded. UKHSA is no different. So just write whatever you wish, or nothing at all but be authentic as it's not right to overrepresent a minority of one (me).
Thanks so much for asking. I'll fix my post, but I don't need you to write back to anyone at all. Just supporting his request with a "like" is sufficient. I think I will remove the request for more info. If Meghan (the person who is likely going to push the agency to include stratification by public interest shown) gets a sense that something or someone is coordinating this request then she might become skeptical of its utility. I don't want to push people who are willing to give the public information, if they can as long as they don't realize in advance that those same data classifications could be detrimental to the public health campaigns current advocated strategy in the future if the numbers show something they didn't expect. This is why we need to get them to include those numbers now before the "trend line" becomes clearer. As you know, when the trend line shows something they didn't expect, they will censor it. So best is to act early for transparency, without malice or agenda. Just data.
OK, got it, thank you for the clarification.
" I'm a better writer than a thinker, and I am absolutely terrible at writing "
:)