
Challenge UKHSA - Reveal Infections/Mortality in recovered Vaccinated
Release this data if you want to prove Vaccine Safety.

Provide Realtime Vaccination Effectiveness For These
Recovered then Vaccinated
Days since injection before SARS-COV-2 positivity
Number of Doses
Effectiveness against Severe Disease
Hospitalization
Death
Days since last positive record
Recovered Never Vaccinated
Days since last infection before SARS-COV-2 positivity
Effectiveness against Severe Disease
Hospitalization
Death
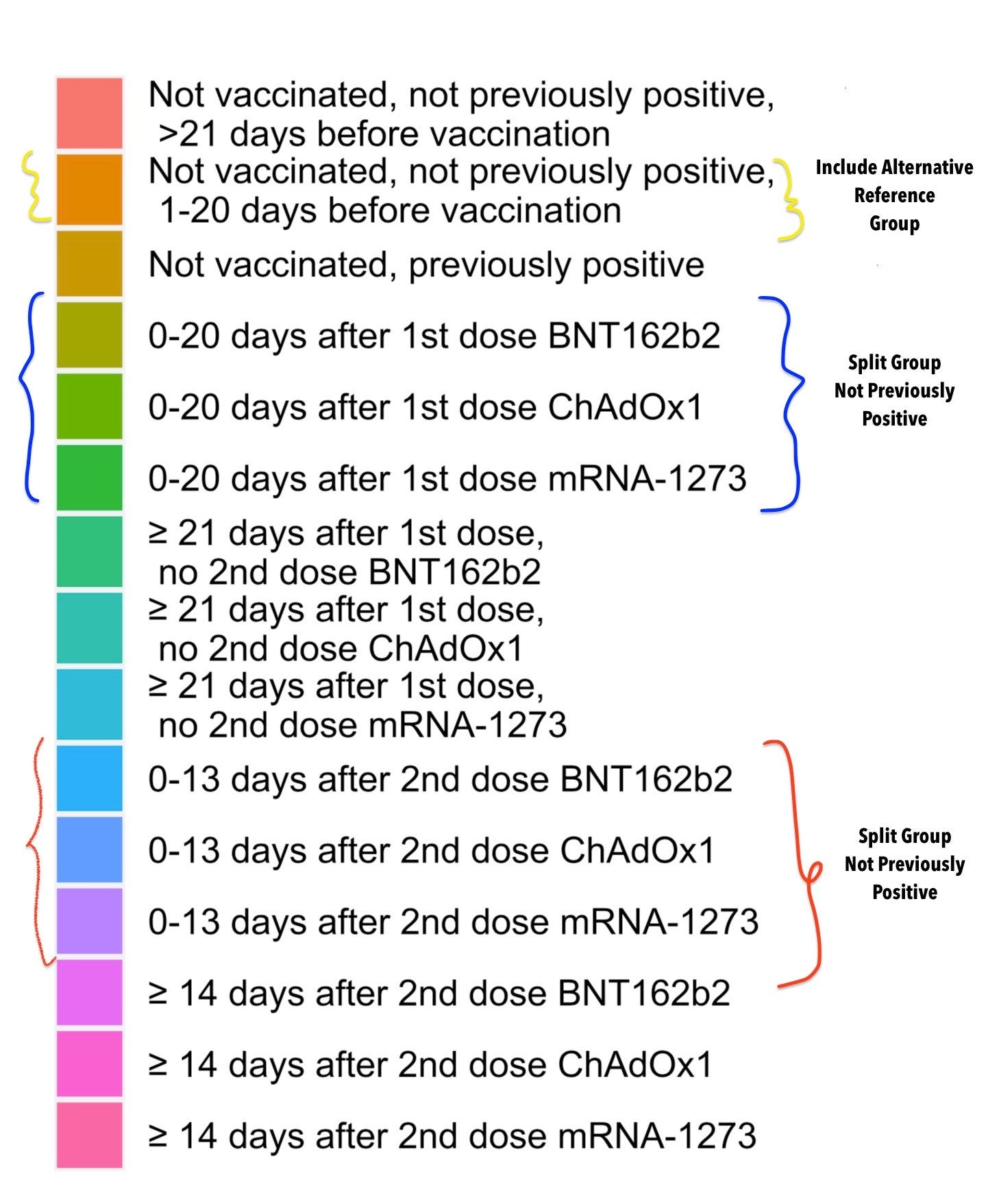
Reference Group should be Unvaccinated not the “Unvaccinated 21 days before”. The Vaccine Effectiveness has to be done like for like, not censoring healthy Unvaccinated people from the reference group to hide negative VE.
This study is not showing the vaccine effectiveness that people actually care about, you are hiding important information by censoring poor outcomes in the days after vaccination and comparing against a different reference group. Malpractice.


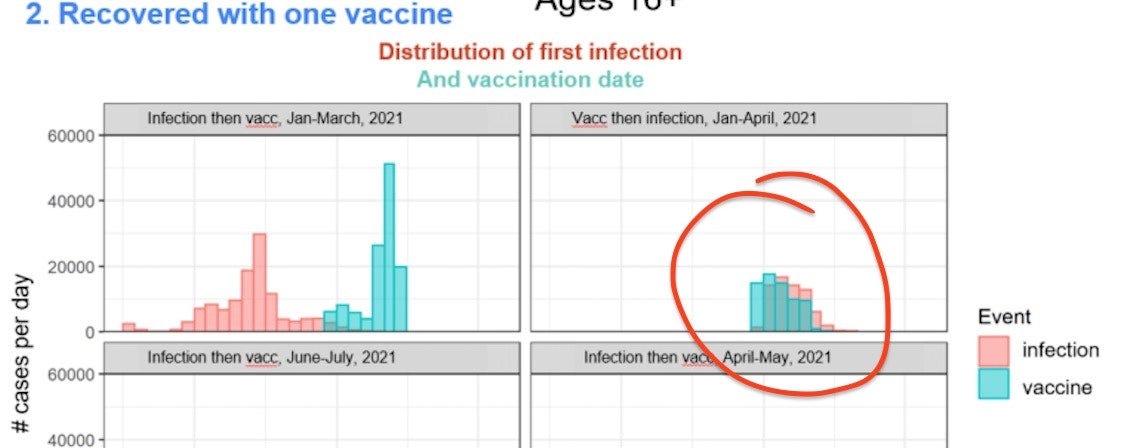
What happened here in Israel? Why does the shape of those curves match so closely. Is this what UK is relabelling as “Reinfection before Vaccination”. Because they should tell us. How many people, and what proof do they have that it was a re-infection?
Pfizer’s own data shows that people with a history of Covid Infection and recent positivity is linked to negative V.E. of 10% to 15% in probably the healthiest participants with just the first dose. It’s -100% VE in seropositive in UK Care Homes in December last year. They never told people that they are at risk. They don’t test people before they administer a vaccine systemically for a respiratory virus. The data is expertly manipulated to always leave out the risk of infection, and disease in the days following vaccination. This has been seen in the UK, and in the Pfizer data. India’s Covaxin also showed almost doubling of cases in treatment arm compared to placebo when both had equal baseline seropositivity. Scottish large observational study of healthcare workers found -10%-13% efficacy of getting vaccinated for those with seropositivity. The list is not long, since this data is extremely hard to find. Why? Because it would stop mass vaccination if people knew that dangers of starting an epidemic in a population that has reached equilibrium and has high seroprevalence and some asymptomatic carriers.
-Now that the crude rates are too high in double vaccinated in UK, we are getting fancy commentary Link to report:
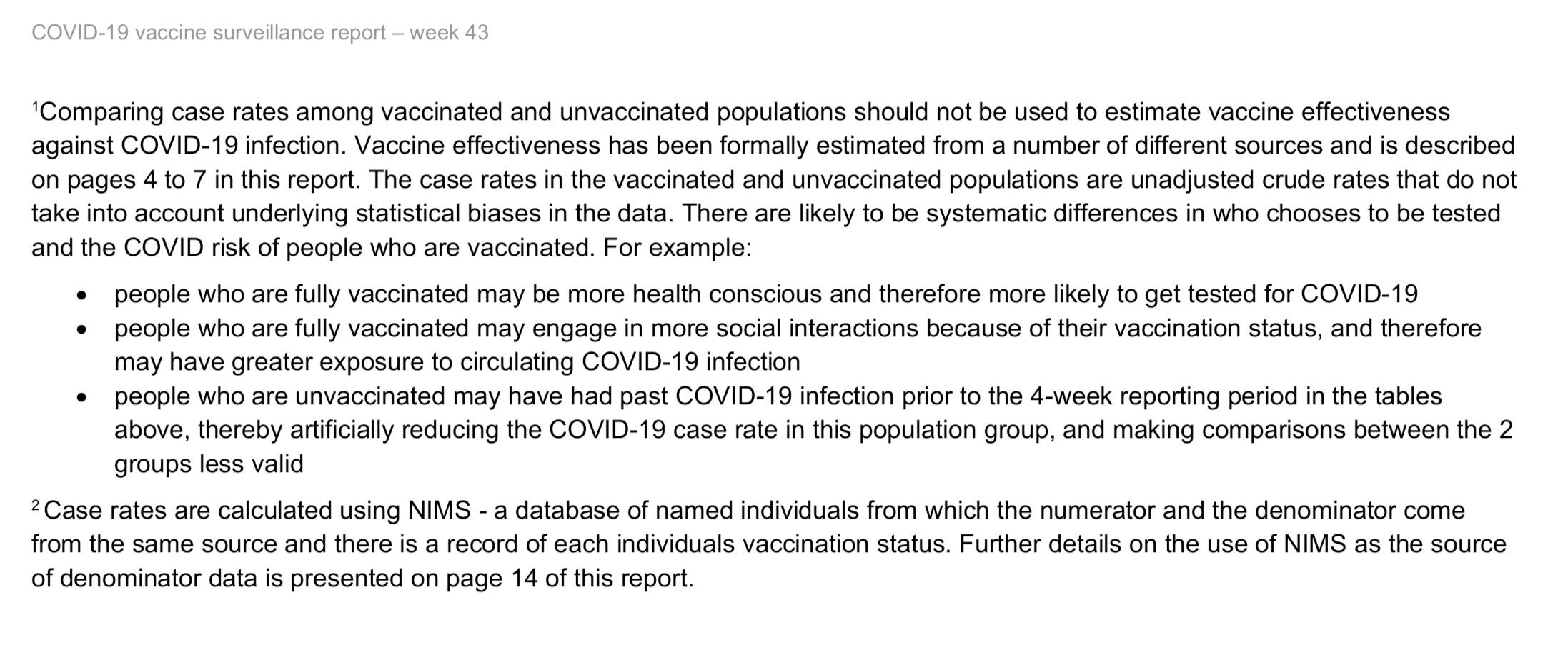
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1029606/Vaccine-surveillance-report-week-43.pdf
1. "The vaccination status of cases, inpatients and deaths is not an appropriate method to assess vaccine effectiveness...[reasons]"
2. "There are likely to be...[hypotheses]"
3. Hypothetical Examples "Maybe []", "may []" then "may []", "may []" + "may []" + "artificially [something]", "less valid".
Point 1. Should be quoted verbatim by all sane and decent people from now on as the official position by a health authority, to help protect the rights of those who are being persecuted without scientific justification. Crude rates [raw data] of Cases, Hospitalizations and Deaths are not appropriate to make assessment about vaccine effectiveness.
Therefore, we should be allowed to dismiss without prejudice anything that relies on raw data or resembles [1] and not be penalized, harassed, banned or forced to consume or repeat that which is "not an appropriate method". This claim by UKHSA should be enough to throw out every disinformation claim against people who refuse to uncritically rely on vaccine effectiveness computations using their personal protocol and deeply held beliefs about what the formula ought to be. They may convince others and are free to do so, but their personal vaccine effectiveness calculations [PVEC] should not be used to decide the fate of others, who neither consented to anyone's reckoning based on someone else's preferred statistical biases/protocol nor did they implicitly agree that some predetermined course of action has to be executed based on these computations of Vaccine Efficacy.
2. UKHSA is pretty good at conjugating the ifs, maybes to weave stories that imply with certainty what the essential qualities of persons who have taken the single action "Get Vaccinated" are likely to be. Based on this previous hypothesis, they have already built another hypothesis that people with vaccination status have greater social access and exposure, not as a confounder but literally "because of their vaccination status". No requirement on their part to follow these up with any commitment to release raw data that shows this, or if they don't have it, then commit to testing it. To use a series of assumptions to imply that crude rates are "less valid" than their hypothesis is just that: A hypothesis. If it's less valid then they should demonstrate it.
They should state clearly: We believe X will do Y at this rate, and we will show this by using the formula X -> Y rate to predict accurately what the crude rate for [whatever they believe] will be tomorrow, day after, in a week. They should do a negative control too, a will not have c amount of whatever in the next 10 days. If UKHSA can accurately predict this, then they will have shown that their hypothesis was true for the time they tested.
They also have access to people's vaccination status. They should predict in advance what number of people will have more social interactions in a one week period. As a sanity check, they should test their rather strong causal claim that "because of vaccination status" rather than some confounder like being vaccinated was more predictive. They can check this easily: Many people in the UK are vaccinated with vaccines not recognized by National Immunization Registries. A person working and vaccinated with first dose in England who has to return home to Scotland is unable to be recognized as Vaccinated before their second dose and Vice-versa. Someone in the UK who has been immunized using a vaccine that is not recognized by WHO, cannot get a vaccination pass or "vaccination status". Is the lack of this recognition truly stopping them from interacting? If they have proof, then they should show it. If what they are saying is true, then it will be easy to do a random sample of people who profess to have vaccination status and find out how many have fake cards. Does a fake immunization status make them more or less prone to exposure?
Finally, if vaccinated people are having more exposure, and vaccinated people are having more interactions. They should come-up with a test to show what this exposure is in a definite way. Not hocus pocus of counting heads, but real epidemiology like Singapore contact tracers. UKHSA can claim that vaccinated have more interactions and more exposure, they do nothing to show that this is the case. They should announce in advance, that they believe vaccinated people are going to have exposure at rate x in so y number of hours. Like Shanghai CDC tested in May 2020, they simply checked what amount of infectious aerosol per unit volume of air exists in various public places. UKHSA can surely do this. Release in advance what the flux density of vaccinated susceptibles has to be so that one unit of unvaccinated person time spent gives R infections. Make this calculation public in advance. Make the case that you are able to predict with certainty what the transmission dynamics will be based on the infections that arise out of an event. Show us that your calculations can look at the macro-infections and predict with certainty the number of unvaccinated people time these susceptible vaccinated must have spent to get infected consistently.
UKHSA will never actually accept this challenge. Evidence free stigmatizing of people is practiced and encouraged. Showing your own homework, before lecturing others and commanding them to not use "less valid" methods is never a possibility. Did the public demand demand that PHE release crude rates from raw figures? No. It was done by UKHSA because they have no problem using "less valid" comparisons as long as it's showing something they don't have to explain. It never occurred to them that hiding one statistic by misdirecting with another will not ultimately serve them or the public. Giving people a false sense of security that you have some grand model that's more valid and that fully predicts the future is immoral. The UKHSA know that they don't have anything. They hardly have raw data and they are worried to release it because they are worried that everyone will find out that haven't a clue what's going to happen and their "statistical biases" are completely useless from a scientific standpoint as it cannot reliably predict what will happen, only confabulate and explain the previous data with "adjusted models" based on adhoc hypotheses that do not have to be tested before being utilized to "control for confounders".
UKHSA, if you are so certain you are not endangering the public by asserting false confidence in the predictive power of your theories, then just announce this to the public: "We will estimate, without even looking at the events in the next week, how many unvaccinated to vaccinated transmissions occurred at a specific event. We will do this using the empirical method alone. We have set-up sensors that will collect droplets and aerosols. We will measure the total ambient infectious viral load in the environment. We will use only the total number of person time spent by accessing registers to measure footfall. Using only samples collected non-invasively and correlating with attendance, we will release the exact number of vaccinated and unvaccinated people that were present in a specific event. We will derive this from just the viral particles in the environment, sewage, air filters, looking at viral load, genomic analysis of virus that could be cultured to find the unvaccinated super spreaders who are disproportionally transmitting to Vaccinated but not the unvaccinated. We will establish the ratio of such persons necessary to explain the transmission rates in Vaccinated. We will then go and verify the identities of people using surveillance footage and CCTV to prove that we know in advance how many such people must exist and must be transmitting to make the breakthrough rates appear higher than the actual which we expect is [whatever they think the actual VE is].
If they cannot even pretend that they have the ability, intention or the cognitive wherewithal to demonstrate their source of confidence in assessing the effectiveness of a tool they have employed, then we shouldn't be instructed as lay people to ignore raw data of cases, hospitalizations and deaths. It's literally the only thing that's somewhat detectable without ambivalence. Death the least bad crude rate.
The UKHSA predicts nothing for the public. Arbitrarily censors raw data [infected 21 days after 2nd dose]. Arbitrarily introduces crude rates at an arbitrary time [when vaccinated deaths were growing larger in absolute terms] but only censors crude rates by vaccination status [rates for 1 dose missing]. Tells people to not conclude a specific conclusion but they conclude other things themselves without any hesitation with no intention to demonstrate. Tell tall tales about the perils of crude rates that might be "artificially reducing" while doing nothing themselves to prove this "artificiality" by releasing raw numbers and predicting.
In short, no raw data for the public to try to asses what hazards await them. Selectively releasing raw data and presenting the data in crude rates which is "less valid" for almost 1 year. If someone tries to infer whatever they could from whatever is released. They are told not try as it's wrong. UKHSA is confident that all is well. Vaccine Effectiveness has a secret formula, and the data is secret anyway, so there is no point in releasing it to the public. Makes sense. Tell people that they are fine. All is well. No need for data. We told the public the reality. We know it.
A few unvaccinated lepers must doing the rounds. It must be only a few of these unvaccinated spoiling it because remember, UKHSA thinks that most of unvaccinated people must've been infected already and the rest probably last month, we obviously know that those who had SARS-COV-2 exposure, got vaccinated and are dead, so they couldn't be contributing the Vaccinated's herd immunity.Mostly all that recovered are magically in the unvaccinated and we know that's rigging "less valid". So it's safe to say that only a few in the unvaccinated are getting superpowers of infection then super-spread to vaccinated and vaccinated only, never the unvaccinated. Also, the unvaccinated are getting the infections from the unvaccinated but we can't see it. Trust UKHSA. Since vaccinated people are only susceptible to unvaccinated, and as we know, vaccination stops transmission from vaccinated to vaccinated, it's logical to conclude without needed any empirical evidence that the unvaccinated and gaining access to these social events with high exposure risk that the vaccinated are using "because of the vaccination status". So how do the unvaccinated show up at these posh parties? UKHSA doesn't have to explain that. So to conclude -
Vaccinated are less susceptible.
Vaccinated are seeing each other a lot.
They are at exclusive Vaccinated only parties.
They are getting infected at such a high rate that it looks like they are more susceptible.
But they are not. Because we said so.
We don't have to prove anything. We don't have to predict anything.
The safe and effective vaccines are still working.
If we can remove and disappear the unvaccinated Dracula that's efficiently finding all the vaccinated at these vaccinated only parties day after day is the main phantom driver.
Makes sense, no data needed. Unvaccinated recovered cannot get Covid. Unvaccinated are not getting infected at such a high rate, therefore unvaccinated are all unvaccinated recovered. Every single UK infection must've skipped the Jab, that's why the vaccinated are not getting the protective powers of the infection that they took the jab to avoid. UKHSA maintains that this is the only plausible explanation and other theories are "less valid", like the suggestion that vaccinated are not only getting infected but also infecting others and transmitting the virus. This cannot be true, because unvaccinated are also capable of transmitting and since they can't have social interactions due to vaccination status, infections are only happening in the vaccinated party goers. The unvaccinated are therefore infecting the vaccinated at high rates without being around them and without infecting their unvaccinated pals because they are recovered.
I think UKHSA has this exactly right. They are so right, there is no need to release any numbers anymore. Stop the count. Stop the meaningless selective reporting of raw data that's designed to mislead. Let the people live in complete bliss with all faith into the UKHSA. We have no reason to want to know anything, we trust you.
And no need to ever breakdown the infection rates by vaccinated recovered vs unvaccinated recovered. Especially, never let the public see what the VE for recovered vs recovered then vaccinated is. Especially don't release the crude rates for hospitalization in that category.
No need or time for fairy tales about "why", nobody cares. If the UKHSA thinks something is artificially reduced or increased, good for them. They should release all the raw data that they are withholding and release the natural and true rate calculations. We will see if they are correct or if they are also wrong.
UKHSA. Instead of conjectures and lectures, why don't you either stop feeding selective data/crude rates, and allow the public to assess without supervision, full datasets to verify the the basis of assurances and confidence. It's unethical to tell people that they are safe or not safe without sharing the basis for that judgement and the unadjusted raw data by vaccine Status.
ONS infections survey published a paper that graphed the viral load of people and the column with the highest load was "reinfections before vaccination".
No account was given at all about this alarming finding. No discussion about how it was determined that a "re-infection" (which is an infection, following a previous infection) occurred, let alone how it was determined that it was before vaccination. If it was before vaccination then why did this person decide to vaccinate with an active infection and why would someone allow that, has it been determined to be safe? Where is the data showing that vaccinating a person with an active infection is safe, it's never been shared. What's the V.E. in such persons? V.E. against future infections, V.E. against hospitalization and V.E. against death?
After all UKHSA's "Vaccine effectiveness is not as bad as it looks in crude rates" outlook is built on the pillar that recovered individuals in vaccinated population are far outnumbered by recovered individuals in unvaccinated. Surely then we can be allowed to look at the following unadjusted data?
Never Infected Never Vaccinated - Total - All Cause Mortality - Hospitalizations - Infections
Recovered Never Vaccinated - Total - All Cause Mortality - Hospitalizations - Infections
Reinfected Never Vaccinated - Total - All Cause Mortality - Hospitalizations - Infections
Vaccinated Never Infected - Total - All Cause Mortality - Hospitalizations - Infections
Vaccinated Recovered - Total - All Cause Mortality - Hospitalizations - Infections
Recovered Vaccinated - Total - All Cause Mortality - Hospitalizations - Infections
Reinfected Vaccinated - Total - All Cause Mortality - Hospitalizations - Infections
Notice: We never get Vaccine Effectiveness numbers by the UKHSA in
Recovered then Vaccinated cohort. Ever wondered why? When this cohort is important from a safety and efficacy standpoint. I think they don't want us to know. Reinfected Vaccinated shouldn't be a categorized without genomic sequencing and proof that the infection is a new one. If it cannot be determined, then it should be presented as re-infection or re-activation or chronic infection.
Can UKHSA then adjust all that they want and tell us clearly: What's the VE against infection, hospitalization and death in the first few weeks for a recovered individual vs a recovered individual who got vaccinated.
Also, 2 dose 14 day VE for recovered then vaccinated vs recovered. Just tell us this information. It's not right to hide it systematically.
Let me guess. The Data will not come. Why? Because it will show negative efficacy. The recovered individuals who vaccinate lose their protection against infection by about 10-15%. Prove me wrong. Challenge.